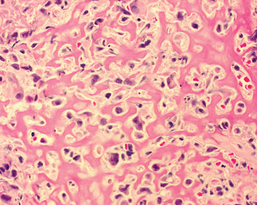
10 Orthopaedic tumors and masses Figure 10-1. A permeative pattern of destruction from a metastatic lesion in the diaphysis of a femur. Figure 10-9. High-power view of osteosarcoma. Malignant cells are evident among the pink bands of osteoid.
Introduction
 Orthopaedic oncology is a field of orthopaedic surgery that specializes in the diagnosis and treatment of both benign and malignant tumors of the bones and soft tissues of the extremities, pelvis, and spine. Although definitions vary, a tumor can be thought of simply as any mass in the soft tissues or bone that otherwise should not be there. For example, a tumor may be a neoplasm, which is an abnormal proliferation of abnormal cells; a hamartoma, which is an abnormal proliferation of normal cells; or simply an infection causing a masslike effect. The focus of this chapter will be the common neoplasms encountered by the musculoskeletal oncologist.
Orthopaedic oncology is a field of orthopaedic surgery that specializes in the diagnosis and treatment of both benign and malignant tumors of the bones and soft tissues of the extremities, pelvis, and spine. Although definitions vary, a tumor can be thought of simply as any mass in the soft tissues or bone that otherwise should not be there. For example, a tumor may be a neoplasm, which is an abnormal proliferation of abnormal cells; a hamartoma, which is an abnormal proliferation of normal cells; or simply an infection causing a masslike effect. The focus of this chapter will be the common neoplasms encountered by the musculoskeletal oncologist.
Malignant bone disease
 There are many categories of malignant neoplasms. Some of these include carcinomas (from epithelial origin), adenocarcinomas (from epithelial cells with secretory properties), lymphomas (arising from lymphocytes), leukemia (from bone marrow cells), and melanomas (from transformed melanocytes). A sarcoma is a malignant neoplasm that arises from cells of mesenchymal origin. Mesenchymal tissues include those found in the limbs and pelvis: bone, cartilage, muscle, fat, vessels, and nerves. Sarcomas are exceedingly rare. Every year in the United States there are fewer than 10,000 new cases of bone sarcoma and fewer than 15,000 new soft tissue sarcomas.
There are many categories of malignant neoplasms. Some of these include carcinomas (from epithelial origin), adenocarcinomas (from epithelial cells with secretory properties), lymphomas (arising from lymphocytes), leukemia (from bone marrow cells), and melanomas (from transformed melanocytes). A sarcoma is a malignant neoplasm that arises from cells of mesenchymal origin. Mesenchymal tissues include those found in the limbs and pelvis: bone, cartilage, muscle, fat, vessels, and nerves. Sarcomas are exceedingly rare. Every year in the United States there are fewer than 10,000 new cases of bone sarcoma and fewer than 15,000 new soft tissue sarcomas.
 Malignant bone disease often causes bone destruction or lysis. A permeative or moth-eaten pattern of lysis (Fig. 10-1), in which the bone is aggressively destroyed with indistinct margins, is usually displayed. A more geographic pattern, in which there is a clear margin between normal and abnormal bone, is seen with benign tumors (Fig. 10-2).
Malignant bone disease often causes bone destruction or lysis. A permeative or moth-eaten pattern of lysis (Fig. 10-1), in which the bone is aggressively destroyed with indistinct margins, is usually displayed. A more geographic pattern, in which there is a clear margin between normal and abnormal bone, is seen with benign tumors (Fig. 10-2).

Metastatic disease
 Metastatic carcinoma to bone is 25 times more likely to occur than primary bone sarcoma. The five primary carcinomas that most commonly metastasize to bone are breast, prostate, lung, kidney, and thyroid. In contrast to the small numbers of primary bone sarcoma, there are more than a million new cases of these five carcinomas in the United States every year. Metastatic carcinoma most commonly occurs in the thoracic and lumbar spine (theoretically because of the valveless Batson”s venous system there) but can occur in virtually any bone. It commonly presents as pain and can lead to weakened bone and pathologic fractures (fractures that occur at normal physiologic loads).
Metastatic carcinoma to bone is 25 times more likely to occur than primary bone sarcoma. The five primary carcinomas that most commonly metastasize to bone are breast, prostate, lung, kidney, and thyroid. In contrast to the small numbers of primary bone sarcoma, there are more than a million new cases of these five carcinomas in the United States every year. Metastatic carcinoma most commonly occurs in the thoracic and lumbar spine (theoretically because of the valveless Batson”s venous system there) but can occur in virtually any bone. It commonly presents as pain and can lead to weakened bone and pathologic fractures (fractures that occur at normal physiologic loads).
 Metastatic breast cancer is common in women with advanced disease. Radiographically, it is classically a mixed lytic and blastic lesion; that is, it causes lysis of bone and formation of bone (Fig. 10-3). It typically responds to radiation therapy but commonly requires surgical stabilization. Metastatic prostate cancer is also radiosensitive but typically is a purely blastic process (Fig. 10-4). Lung, kidney, and thyroid disease usually cause purely lytic and destructive lesions (Fig. 10-5). Renal cell carcinoma and thyroid disease are extremely vascular lesions that often require embolization before open surgical treatment.
Metastatic breast cancer is common in women with advanced disease. Radiographically, it is classically a mixed lytic and blastic lesion; that is, it causes lysis of bone and formation of bone (Fig. 10-3). It typically responds to radiation therapy but commonly requires surgical stabilization. Metastatic prostate cancer is also radiosensitive but typically is a purely blastic process (Fig. 10-4). Lung, kidney, and thyroid disease usually cause purely lytic and destructive lesions (Fig. 10-5). Renal cell carcinoma and thyroid disease are extremely vascular lesions that often require embolization before open surgical treatment.
 Because of the overwhelming preponderance of potentially metastatic carcinoma, any lytic bone lesion in a patient older than 40 years of age should be considered metastatic disease until proven otherwise. Workup for these patients should include radiographs of the entire affected bone, magnetic resonance imaging (MRI) of the area to assess soft tissue extent, a bone scan to assess other skeletal disease, and a computed tomography (CT) scan of the chest, abdomen, and pelvis in an attempt to identify the primary site (Fig. 10-6). Often a biopsy will still be necessary to secure a definitive tissue diagnosis.
Because of the overwhelming preponderance of potentially metastatic carcinoma, any lytic bone lesion in a patient older than 40 years of age should be considered metastatic disease until proven otherwise. Workup for these patients should include radiographs of the entire affected bone, magnetic resonance imaging (MRI) of the area to assess soft tissue extent, a bone scan to assess other skeletal disease, and a computed tomography (CT) scan of the chest, abdomen, and pelvis in an attempt to identify the primary site (Fig. 10-6). Often a biopsy will still be necessary to secure a definitive tissue diagnosis.
Multiple myeloma
 Multiple myeloma, a malignant disease of monoclonal plasma cells, is the second most common cause of lytic lesions in adults. It is more common in men in their 60s and in African Americans. The bone lesions are well-defined, punched-out lytic areas that can be seen in any bone (Fig. 10-7) and are often seen in the skull. Patients will often have anemia (from bone marrow replacement by tumor), hypercalcemia (from the bone lysis), and a monoclonal protein spike on urine and serum protein electrophoresis. Treatment is multimodal, requiring medical oncology, radiation oncology, and orthopaedics.
Multiple myeloma, a malignant disease of monoclonal plasma cells, is the second most common cause of lytic lesions in adults. It is more common in men in their 60s and in African Americans. The bone lesions are well-defined, punched-out lytic areas that can be seen in any bone (Fig. 10-7) and are often seen in the skull. Patients will often have anemia (from bone marrow replacement by tumor), hypercalcemia (from the bone lysis), and a monoclonal protein spike on urine and serum protein electrophoresis. Treatment is multimodal, requiring medical oncology, radiation oncology, and orthopaedics.
Lymphoma
 Metastatic disease and multiple myeloma account for the vast majority of malignant lesions of bone in adults and should be the first and second entities on any differential diagnosis. Lymphoma that arises primarily in bone, although rare, can also be seen. It is often in younger and middle-age adults and classically has a large soft tissue mass with little bony change or destruction. Surgery for lymphoma of bone is for biopsy and bone stabilization only; definitive treatment with high cure rates is a combination of chemotherapy and radiation.
Metastatic disease and multiple myeloma account for the vast majority of malignant lesions of bone in adults and should be the first and second entities on any differential diagnosis. Lymphoma that arises primarily in bone, although rare, can also be seen. It is often in younger and middle-age adults and classically has a large soft tissue mass with little bony change or destruction. Surgery for lymphoma of bone is for biopsy and bone stabilization only; definitive treatment with high cure rates is a combination of chemotherapy and radiation.
Primary sarcoma of bone
 Except for chondrosarcoma (which is seen almost exclusively in adults) the primary sarcomas of bone occur more commonly in the pediatric population. Therefore, entities like osteosarcoma and chondrosarcoma should be considered at the bottom of the differential diagnosis of malignant bone lesions in adults (behind metastatic disease, multiple myeloma, and lymphoma). Primary sarcoma should be at the top of the differential diagnosis of aggressive lesions in children. The primary sarcomas below account for the most common entities.
Except for chondrosarcoma (which is seen almost exclusively in adults) the primary sarcomas of bone occur more commonly in the pediatric population. Therefore, entities like osteosarcoma and chondrosarcoma should be considered at the bottom of the differential diagnosis of malignant bone lesions in adults (behind metastatic disease, multiple myeloma, and lymphoma). Primary sarcoma should be at the top of the differential diagnosis of aggressive lesions in children. The primary sarcomas below account for the most common entities.
Osteosarcoma
 Osteosarcoma is the most common primary sarcoma of bone. It is a high-grade disease that has a bimodal age distribution; it arises mostly in children but also in the elderly (often secondary to a preexisting condition like Paget”s disease). It can occur in any bone but is most common around the knee. Radiographically, it is classically a mixed lytic and blastic lesion with a soft tissue mass characterized by a “sunburst,” radial pattern of osteoid formation (Fig. 10-8). Pathologically, the tumor is required to have malignant cells producing osteoid (Fig. 10-9).
Osteosarcoma is the most common primary sarcoma of bone. It is a high-grade disease that has a bimodal age distribution; it arises mostly in children but also in the elderly (often secondary to a preexisting condition like Paget”s disease). It can occur in any bone but is most common around the knee. Radiographically, it is classically a mixed lytic and blastic lesion with a soft tissue mass characterized by a “sunburst,” radial pattern of osteoid formation (Fig. 10-8). Pathologically, the tumor is required to have malignant cells producing osteoid (Fig. 10-9).
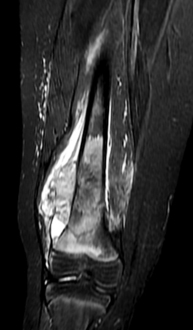
 The workup for osteosarcoma should include an MRI of the entire bone to assess tumor extent (Fig. 10-10), assist with preoperative planning, and rule out any skip metastases (anatomically separate areas of tumor in the same bone); a CT scan of the chest to evaluate the lungs for metastatic disease (the most common site); and a bone scan to evaluate the skeleton (the second most common site of metastatic disease). A biopsy performed by the treating physician is the next step to secure the diagnosis.
The workup for osteosarcoma should include an MRI of the entire bone to assess tumor extent (Fig. 10-10), assist with preoperative planning, and rule out any skip metastases (anatomically separate areas of tumor in the same bone); a CT scan of the chest to evaluate the lungs for metastatic disease (the most common site); and a bone scan to evaluate the skeleton (the second most common site of metastatic disease). A biopsy performed by the treating physician is the next step to secure the diagnosis.
 Treatment for osteosarcoma is typically multidrug chemotherapy, followed by wide excision of the lesion (80% to 90% of cases are limb salvage; see Fig. 10-11), followed by more chemotherapy. Five-year survival rates are currently approaching 80%. Chemotherapy can have ototoxic and cardiotoxic side effects.
Treatment for osteosarcoma is typically multidrug chemotherapy, followed by wide excision of the lesion (80% to 90% of cases are limb salvage; see Fig. 10-11), followed by more chemotherapy. Five-year survival rates are currently approaching 80%. Chemotherapy can have ototoxic and cardiotoxic side effects.
Ewing’s sarcoma
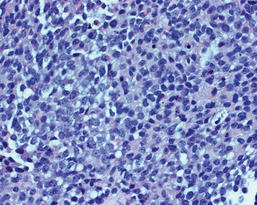
 Ewing’s sarcoma is the second most common primary sarcoma in children. Pathologically, it is a high-grade tumor composed of monotonous, small round blue cells (Fig. 10-12). The majority of Ewing”s sarcomas have a characteristic t(11,22) translocation that results in the formation of the EWS-FLI1 oncogene.
Ewing’s sarcoma is the second most common primary sarcoma in children. Pathologically, it is a high-grade tumor composed of monotonous, small round blue cells (Fig. 10-12). The majority of Ewing”s sarcomas have a characteristic t(11,22) translocation that results in the formation of the EWS-FLI1 oncogene.
 Ewing’s sarcoma is often seen in flat bones and the metaphyseal-diaphyseal regions of long bones. Classically, it has an “onion skin” appearance (multiple thin layers of periosteal reaction at the site of the tumor; see Fig. 10-13). The workup for Ewing sarcoma is the same as for osteosarcoma, but the prognosis is slightly worse. Treatment involves chemotherapy and local treatment. Most tumors are surgically excised, but because Ewing sarcoma is sensitive to radiation, it can be used to treat tumors that are otherwise unresectable.
Ewing’s sarcoma is often seen in flat bones and the metaphyseal-diaphyseal regions of long bones. Classically, it has an “onion skin” appearance (multiple thin layers of periosteal reaction at the site of the tumor; see Fig. 10-13). The workup for Ewing sarcoma is the same as for osteosarcoma, but the prognosis is slightly worse. Treatment involves chemotherapy and local treatment. Most tumors are surgically excised, but because Ewing sarcoma is sensitive to radiation, it can be used to treat tumors that are otherwise unresectable.
Orthopaedic tumors and masses