Open Reduction and Internal Fixation of Ulnar Styloid, Head, and Metadiaphyseal Fractures
Eon K. Shin
Peter Goljan
DEFINITION
Fractures of the distal ulna are often inadequately treated in comparison to its larger counterpart, the radius (FIG 1B,C).
ANATOMY
The radius rotates around the ulnar head through the distal radioulnar joint (DRUJ) during forearm pronation and supination.6, 7
This joint is connected to the carpus by a complicated ligament apparatus, the triangular fibrocartilage complex (TFCC).
The stability of the DRUJ is achieved through bony congruity between the sigmoid notch of the radius and the ulnar head supported by the radioulnar ligaments1, 6 (FIG 2B).
The spheres of the two articular surfaces differ (FIG 2C).
Sixty percent of the joint surfaces are in contact in neutral forearm position.1
In full pronation and supination, there is only 10% bony contact.1
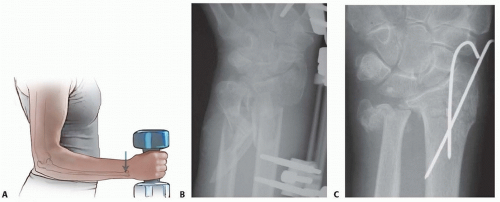
FIG 1 • A. The distal ulna is the fixed point on which performance of most daily hand activities depends. B,C. Fractures of the distal ulna are often neglected in comparison to those of its larger counterpart, the radius, which always attracts attention and treatment efforts. The outcome after distal forearm fractures could be improved if the fixed point—the distal ulna—is addressed surgically at the same time as the radius is operated on.
PATHOGENESIS
Isolated ulnar fractures most commonly occur when the forearm is struck by an object, explaining the eponym “nightstick fracture.”
Distal ulnar fractures are most often due to a fall on an outstretched hand.
It is a common understanding that ulnar-sided injuries are more often caused by falls backward in which the forearm is in supination, loading the ulnar side of the distal forearm and wrist and causing distal ulnar fractures, triquetral chip fractures, TFCC injuries, and so forth.
In contrast, radial-sided injuries are more often caused by falls forward, loading the radial side of the forearm and wrist and causing scaphoid fractures, distal radius fractures, and so forth.
NATURAL HISTORY
Many distal ulnar fractures leave only marginal long-term problems.
Some distal ulnar malunions cause DRUJ incongruency with subsequent instability or blocked forearm rotation (FIG 3). This is why management of these deceptive fractures is important.
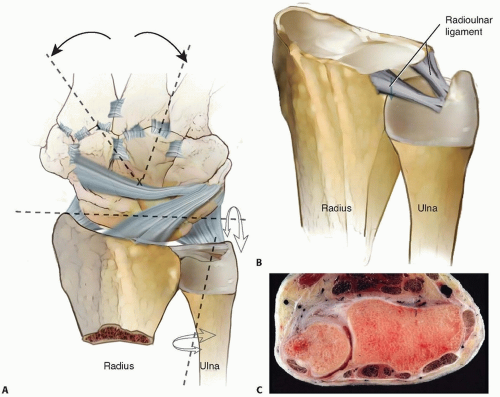
FIG 2 • A. The distal ulna is the fixed point around which the radius rotates in pronation and supination. Through the ulnocarpal ligaments, the distal ulna relates to the hand, allowing daily hand activities. B. The DRUJ is stabilized through the bony congruity between the ulnar head and the sigmoid notch on the radius as well as the dorsal and volar radioulnar ligaments. The radioulnar ligaments include dorsal and volar components that originate on the margins of the sigmoid notch and insert into the fovea and at the base of the ulnar styloid. These ligaments act as reins in the pronation and supination. C. The spheres of the two articular surfaces differ: the ulnar head has a shorter radius of curvature compared with the sigmoid notch.
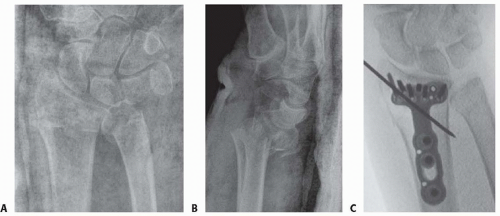
FIG 3 • A,B. Radiographs showing a distal radius fracture together with an ulnar head and styloid fracture. The complexity of the ulnar-sided injury was underappreciated. C. Intraoperative fluoroscopic image after fixation of the distal radius fracture, revealing displaced and unstable ulnar fractures. (continued)
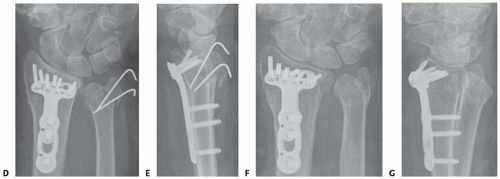
FIG 3 • (continued) D,E. The distal radius fracture was stabilized using a volar locking plate. The ulnar head and styloid fractures were partially reduced and fixed with two Kirschner wires. The surgeon adequately secured the ulnar styloid fracture but not the ulnar head fracture and postoperatively did not restrict forearm rotation. F,G. These radiographs reveal the eventual ulnar head malunion that resulted in DRUJ instability and diminished forearm rotation. The situation was salvaged using an ulnar head replacement prosthesis.
DRUJ stability is an important treatment goal.
IMAGING AND OTHER DIAGNOSTIC STUDIES
Posteroanterior, lateral, and oblique radiographs typically reveal the pathology.
Computed tomography (CT) is useful in examining articular fractures of the ulnar head.
Magnetic resonance imaging (MRI) can be used to evaluate the integrity of the TFCC.
Arthroscopy should be considered if a radiograph leads the physician to suspect DRUJ dissociation without radiographic explanations, such as a displaced ulnar styloid base fracture.
Diagnostic arthroscopy prior to excision of an ulnar styloid nonunion can be useful to evaluate TFCC integrity.16
SURGICAL MANAGEMENT
Findings and Indications
Distal Radioulnar Joint Dissociation
Radiographs occasionally reveal DRUJ dissociation in the absence of an ulnar-sided fracture (FIG 4). This results from detachment of the radioulnar ligament12 (FIG 5A).
Such radioulnar ligament injuries have been found to cause DRUJ laxity and a worse outcome after distal radius fractures in patients without osteoporosis11 (FIG 5B).
Arthroscopically assisted repair or open repair and reattachment of the radioulnar ligament to the fovea of the ulnar head are required to restore stability in the DRUJ (FIG 5C).
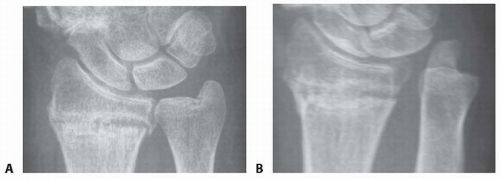
FIG 4 • A. An undisplaced distal radius fracture with no obvious distal ulna pathology. B. The same fracture with a stress test to the DRUJ, and an obvious DRUJ dissociation is seen as a sign of a complete radioulnar ligament detachment in the absence of an ulnar styloid fracture.
Ulnar Styloid Fractures
The importance of ulnar styloid fractures and the need for operative intervention depends on the involvement of the radioulnar ligament insertion site around the fovea of the ulnar head at the base of the styloid (FIG 6A).
Recent literature has demonstrated satisfactory outcomes of distal radius and ulna fractures in which the ulna was left unaddressed following radius fixation.3, 10, 20
An ulnar styloid nonunion was not demonstrated to cause postoperative ulnar-sided wrist pain.20
Adequate demonstration of DRUJ stability is essential during treatment.
If a fracture at the base of the ulnar styloid is displaced more than 2 mm, careful assessment of DRUJ stability is necessary and operative treatment may be required13 (FIG 6B,C).Related posts:
 Operative Treatment of Finger Carpometacarpal Joint Fracture-Dislocations
Operative Treatment of Finger Carpometacarpal Joint Fracture-Dislocations
 Intramedullary and Dorsal Plate Fixation of Distal Radius Fractures
Intramedullary and Dorsal Plate Fixation of Distal Radius Fractures
 Hemiarthroplasty for Proximal Humerus Fractures
Hemiarthroplasty for Proximal Humerus Fractures
 Open Reduction and Internal Fixation of the Posterior Wall of the Acetabulum
Open Reduction and Internal Fixation of the Posterior Wall of the Acetabulum
 Open Reduction and Internal Fixation of Peritrochanteric Hip Fractures
Open Reduction and Internal Fixation of Peritrochanteric Hip Fractures
 Open Reduction and Internal Fixation of Jones Fractures
Open Reduction and Internal Fixation of Jones Fractures

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


