Open Reduction and Internal Fixation of Posterior Wall Acetabular Fractures
Introduction
Classification
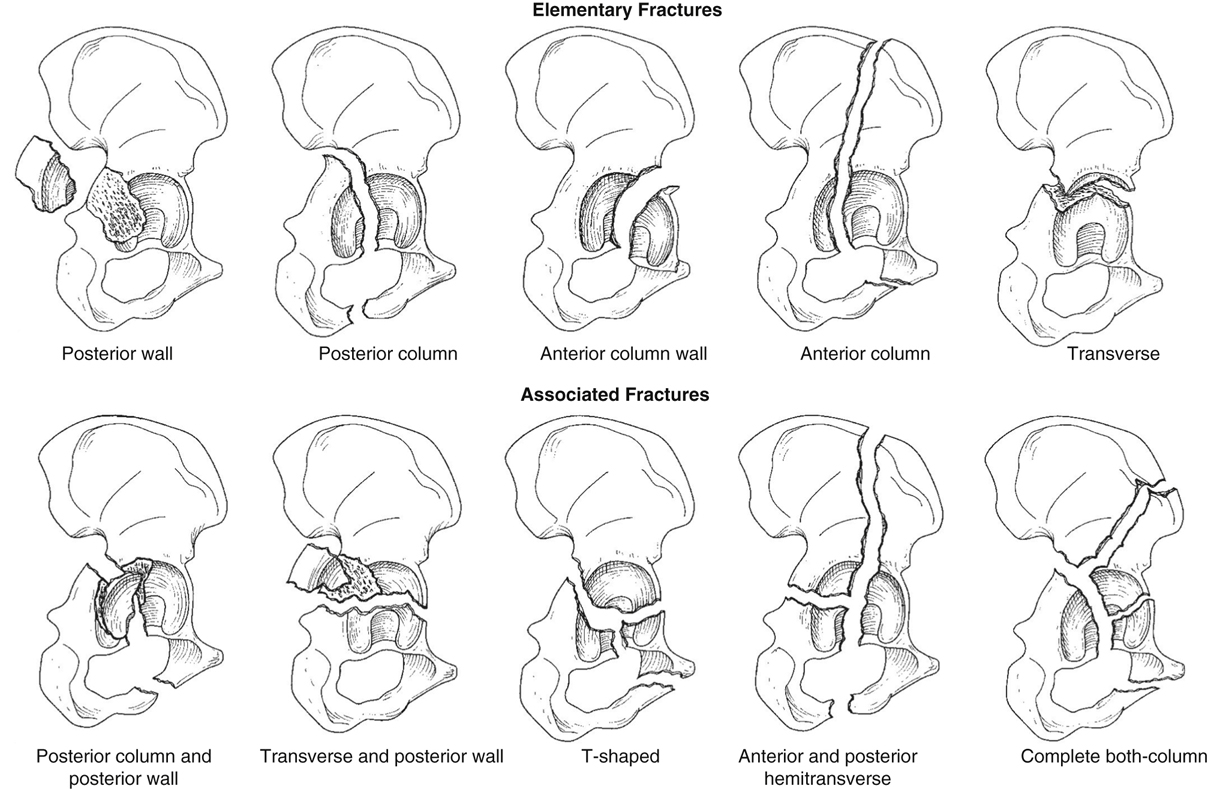
Figure 1Illustrations show the Letournel classification of acetabular fractures.
Letournel classified acetabular fractures into two fracture groups: elementary and associated (Figure 1)
Each group has five types (Figure 1)
Posterior wall fractures are most common type of acetabular fracture, accounting for 25% to 33%
Associated Injuries
Posterior wall fractures result from high-energy trauma; are associated with other serious injuries
Mechanism of injury—Axial femoral loading with hip in flexed position (eg, knee strikes dashboard)
Amount of abduction or adduction of hip at time of impact determines size of posterior wall fragment
Upon displacement of posterior wall fragment, unconstrained femoral head subluxates or dislocates posteriorly in 78% to 86% of cases
Marginal impaction of fractured acetabular articular surface occurs in 27% to 46% of posterior wall fractures
Other associated injuries—Femoral head, neck, and shaft fractures; multiligamentous knee injuries
 | Video 71.1 Posterior Wall Fracture-Dislocation: Reduction and Traction Pin Placement. Lawrence X. Webb, MD; John M. Tabit, DO (4 min) |
Preoperative Imaging
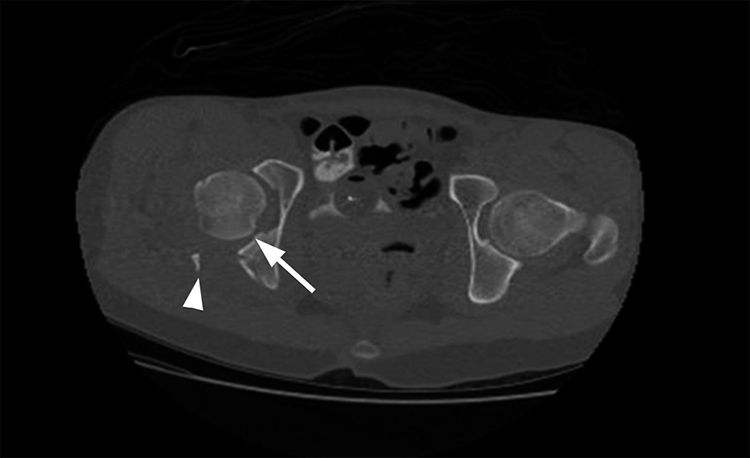
Figure 2Axial CT scan of the pelvis clearly shows a marginal impaction fracture (arrow). The arrowhead indicates the edge of the posterior wall fragment.
AP pelvic radiographs typically show fracture
Judet oblique views, particularly obturator oblique, enable further visualization and classification
CT helps assess femoral head, size and extent of segmentation or comminution of posterior wall fragment, and size and location of intra-articular fragments and marginal impaction fractures (Figure 2)
Procedure
Equipment/Implants
Self-retaining Charnley retractor
Schanz pins (5.0-mm), hand chuck, small femoral distractor
Sciatic nerve retractor, cobra retractor, Taylor retractor
Adhesive plastic strips to temporarily hold retractors
Standard and pituitary rongeurs to extract joint fragments and debris
Cancellous bone allograft or bone graft substitute
Ball-spike pusher
1.5- and 2.0-mm Kirschner wires
Spring plates
3.5-mm reconstruction plates, corresponding aluminum templates, plate benders
C-arm placed on side opposite surgeon
Early Management of Dislocation
Timely reduction of dislocated hip important for pain relief and femoral head blood flow (dislocated longer than 12 hours has adverse effect)
Perform reduction with conscious sedation in emergency department or with general anesthetic and muscle relaxant in operating room
After reducing hip and verifying reduction radiographically, consider keeping knee in extension with knee immobilizer or splint if stable; use skeletal traction if reduction unstable with displaced or intra-articular fragments
Preoperative Planning and Patient Positioning
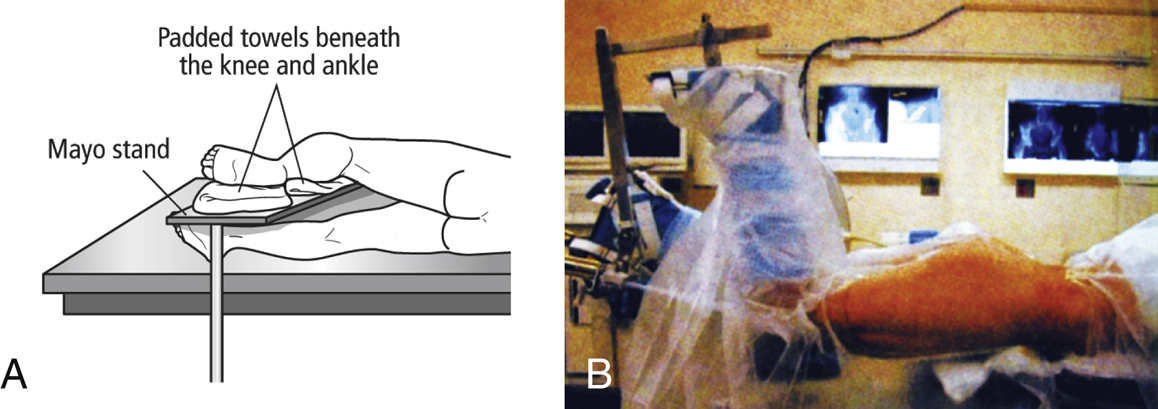
(Panel B reproduced with permission from Siegel J, Templeman DC : Open reduction and internal fixation of the posterior wall of the acetabulum, in Tornetta P III, Williams GR, Ramsey ML, Hunt TR III, Wiesel SW, eds: Operative Techniques in Orthopaedic Trauma Surgery. Philadelphia, PA, Lippincott Williams & Wilkins, 2011, pp 315-325.)
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


