Open Reduction and Internal Fixation of Fracture-dislocations of the Tarsometatarsal Joint
Patient Selection
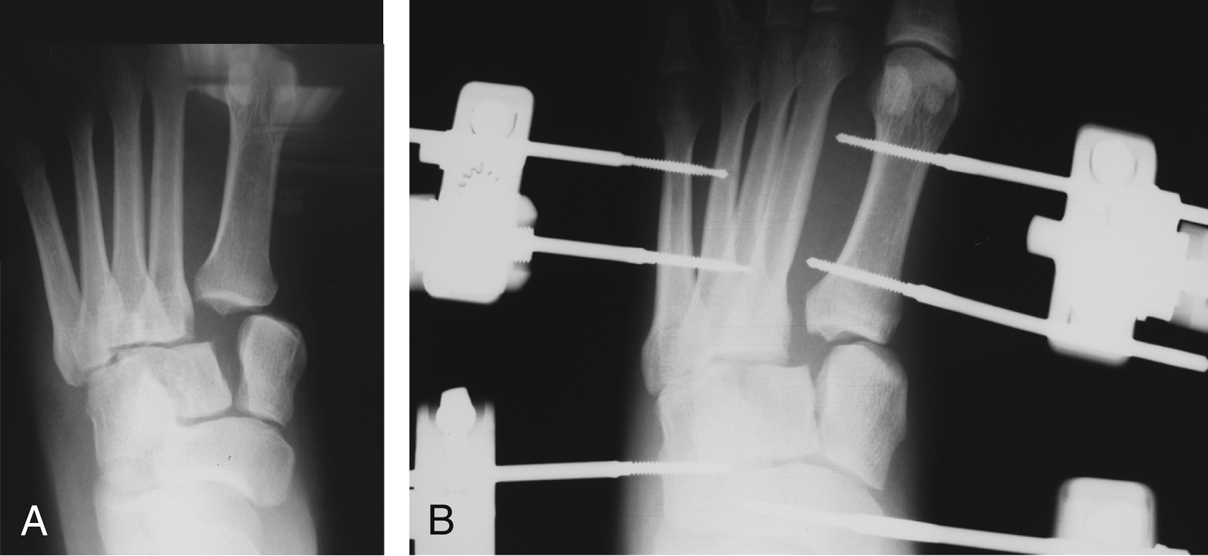
Figure 1AP radiographs show tarsometatarsal joint injury before (A) and after (B) provisional external fixation.
Midfoot fracture-dislocations (Lisfranc)
Most common mechanism is axial load to hyper plantarflexed foot
TMT injuries easily missed; up to 20% missed or misdiagnosed; poor results if treated inappropriately: chronic joint instability, persistent pain, deformity, midfoot arthritis
Indication for open reduction and internal fixation (ORIF) is TMT injuries with displacement and instability
Contraindications include active infection, vascular insufficiency
Consider delaying ORIF for massive midfoot edema; can reduce, provisionally fix with percutaneous pinning or external fixator to prevent skin necrosis, allow soft-tissue recovery (Figure 1)
Plantar ecchymosis can be pathognomonic of high-grade midfoot injury
Diagnostic Imaging
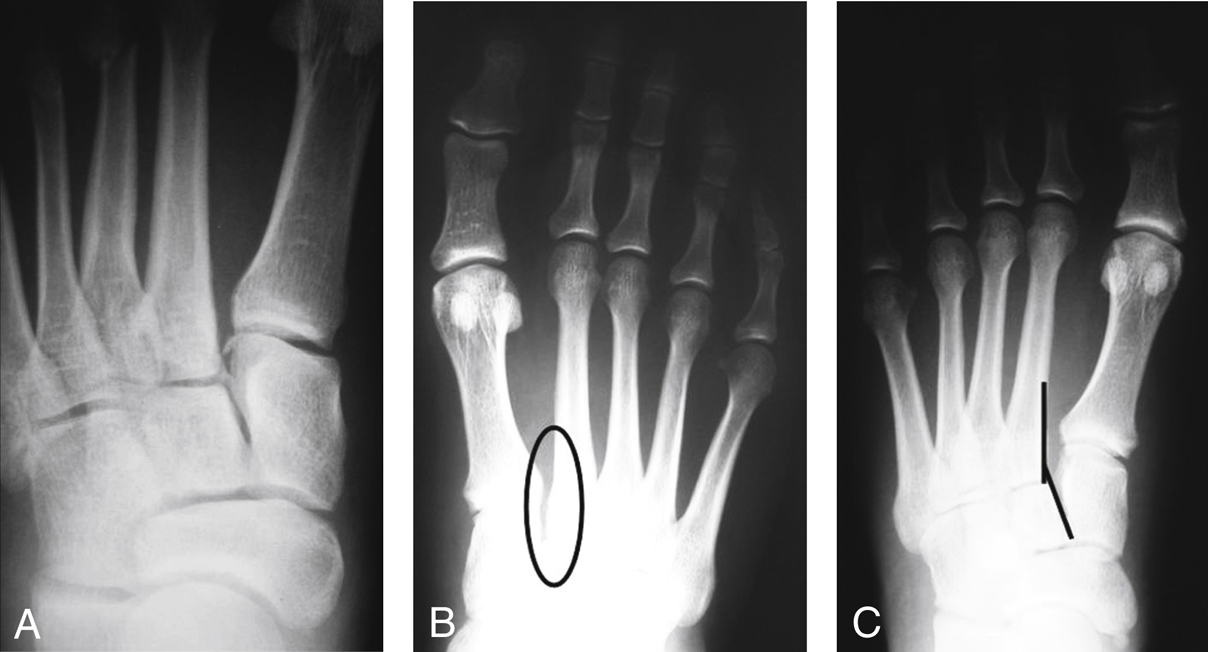
Figure 2Radiographs of a patient with unstable midfoot injury of the left foot. A, In non–weight-bearing radiograph of left foot, injury is not apparent. B, Unaffected contralateral foot (oval). C, Weight-bearing radiograph of left foot demonstrates diastasis (lines).

Figure 3AP radiograph of the left foot shows the fleck sign.
Weight-bearing AP, lateral, oblique views; non–weight-bearing radiographs have 50% misdiagnosis rate (Figure 2)
On AP, assess first, second TMT joints for fracture and diastasis
On oblique, assess for lateral column alignment
Fleck sign (small bone avulsion) can indicate unstable injury (Figure 3)
If plain radiographs not diagnostic, consider stress radiographs, CT, MRI
Stress radiographs performed under anesthesia; can define diastasis at TMT joints
CT helps identify associated fractures, extent of joint injury
MRI can identify Lisfranc ligament tear
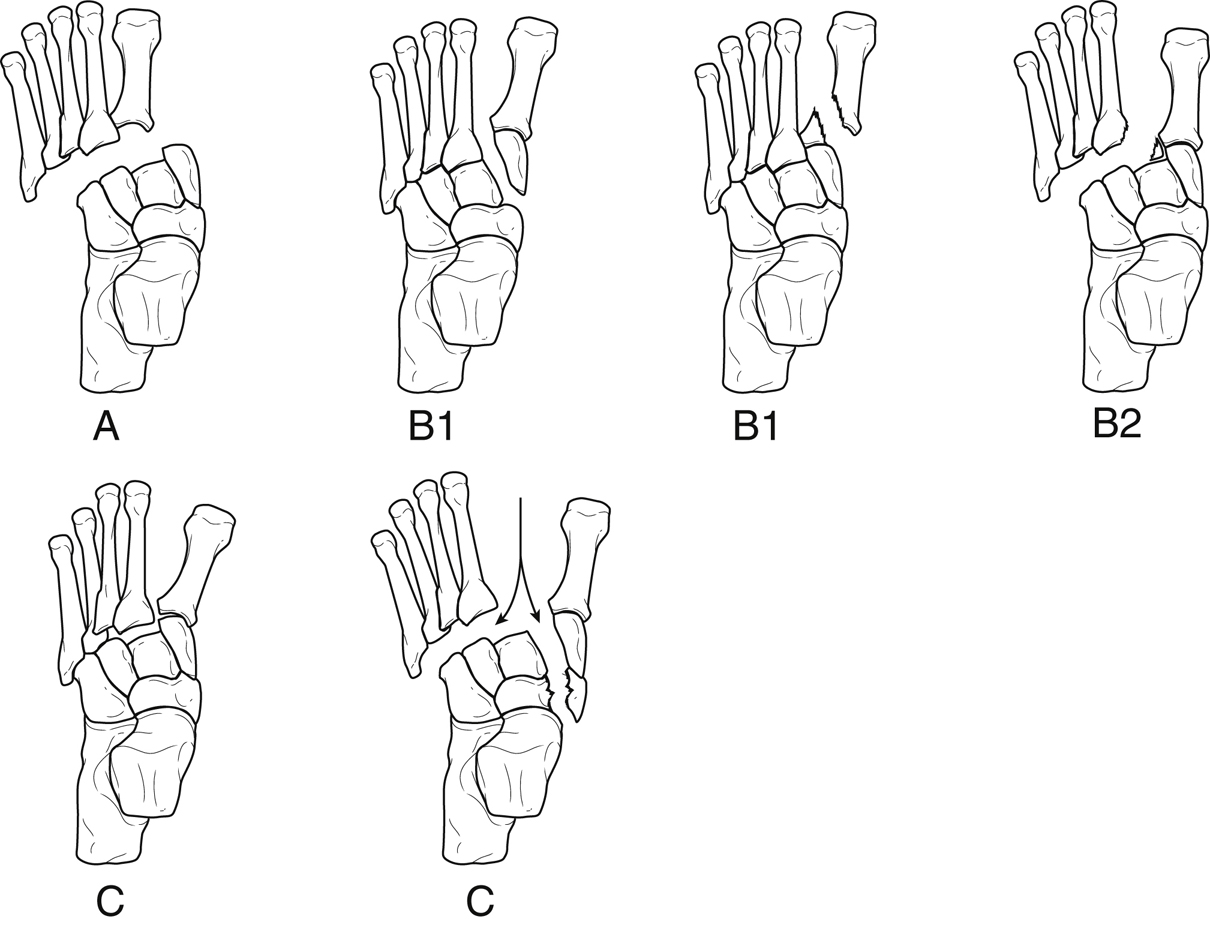
Current classification systems focus on mechanisms, patterns of displacement (Figure 4)
Procedure
Room Setup/Patient Positioning
Supine position with bump under ipsilateral hip
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


