Open Reduction and Internal Fixation of Forearm Fractures
Introduction
The forearm serves as the origin/insertion for muscle groups that control the elbow, wrist, and hand; as well as intrinsic forearm pronation and supination
When injured, anatomic restoration is mandatory for satisfactory function
Fracture predominant in the younger population; average age 35 years
Patient Selection
Open reduction and internal fixation (ORIF) is the standard of care to achieve stable, rigid, anatomic fixation, and best functional outcome
Anatomic realignment of proximal and distal radioulnar joints must be achieved to preserve pronation and supination
Restoring radial/ulnar diaphyseal length and rotation aids restoration of articular alignment by indirect means
ORIF enables early range of motion (ROM) and faster recovery; avoids stiffness, muscular deconditioning, skin atrophy, and potential complex regional pain syndrome
Few contraindications to ORIF exist, but include severe contamination and burns; can use temporary stabilization with external fixator until soft tissues allow rigid fixation
Evaluation
Common mechanisms of injury—Direct blow, fall, gunshot injury
Symptoms—Pain, swelling, tenderness, inability to use forearm
Carefully examine for wounds indicating open fracture
Thoroughly examine and document sensory, motor, and circulatory status
Preoperative Imaging
Obtain AP, lateral, and oblique radiographs
Include joint above and below
Note displacement, comminution, foreign materials, or subcutaneous air
CT/MRI are rarely needed for diagnosis
Preoperative Planning
Includes accurate drawing of fracture, details of fracture position, and location of implants; indicate screw placement
List all needed equipment; note necessary implants and order of use to ensure procurement
Consider dressing supplies, splint/cast material, and preoperative antibiotics
Procedure
Room Setup/Patient Positioning

Figure 1Photographs show the room setup and patient positioning for open reduction and internal fixation of a both-bone forearm fracture. A, The room setup, with C-arm, back table, and instruments prepared. B, The patient is positioned supine on the operating table with the injured arm supported on an arm table.
Supine position; extend arm on arm table (Figure 1)
Tourniquet use recommended
Always include a time out before start of the procedure
Surgical Technique
Exsanguinate extremity with Esmarch wrap; inflate tourniquet to 100 to 125 mm Hg above systolic blood pressure
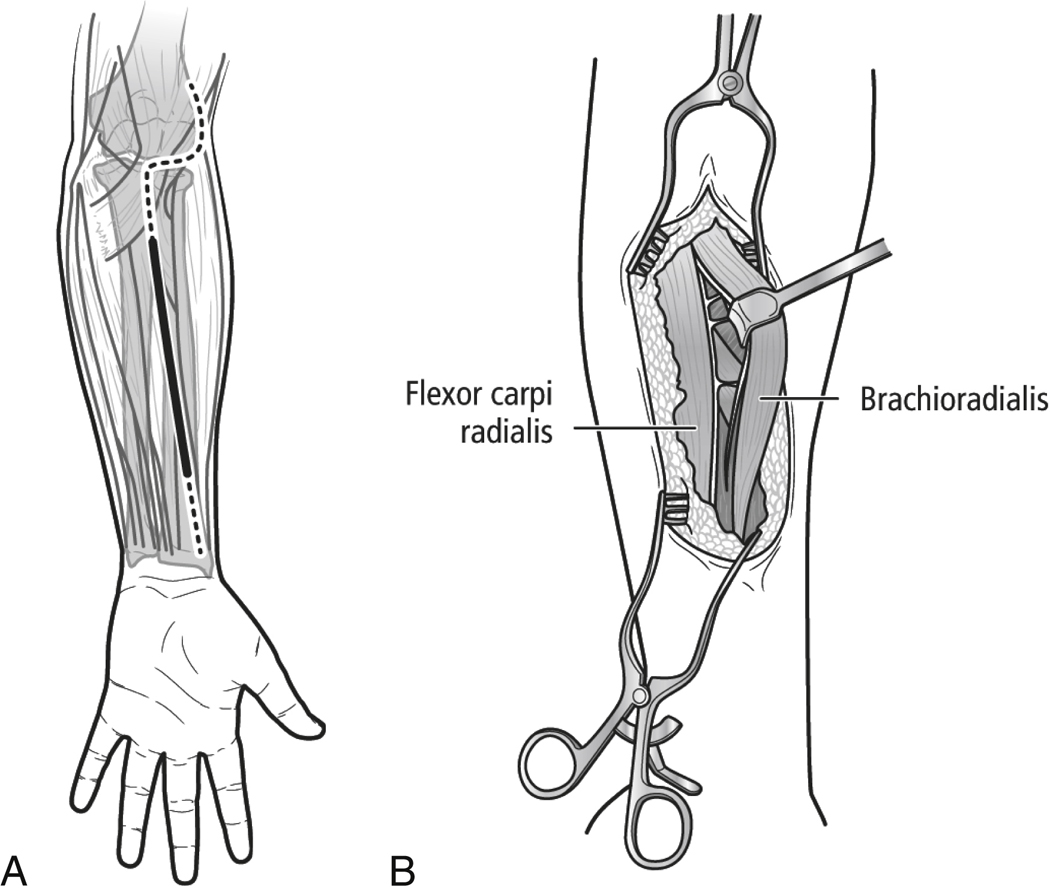
Fracture determines approach; authors use volar approach of Henry for radius (Figure 2) and ulnar midline approach for ulna; for more proximal fractures of the radius, dorsal Thompson approach may be considered
Addressing simpler fracture first aids fixation of more complex fracture
Approach for Radial Fixation
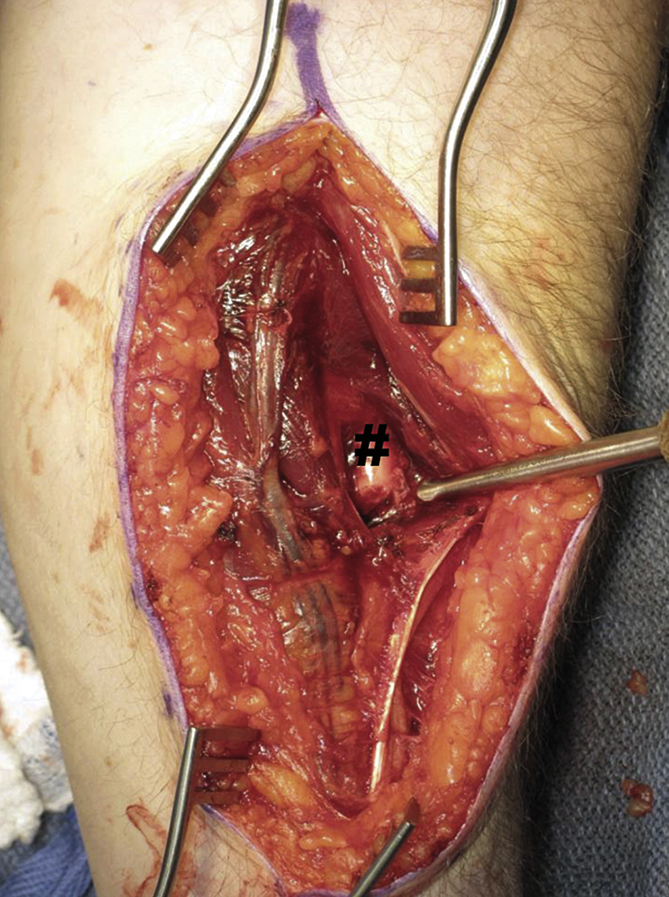
Figure 3Intraoperative photograph shows proximal dissection for open reduction and internal fixation of a both-bone fracture. The brachioradialis and pronator teres muscles are retracted, exposing the fracture, which is denoted by the # sign.
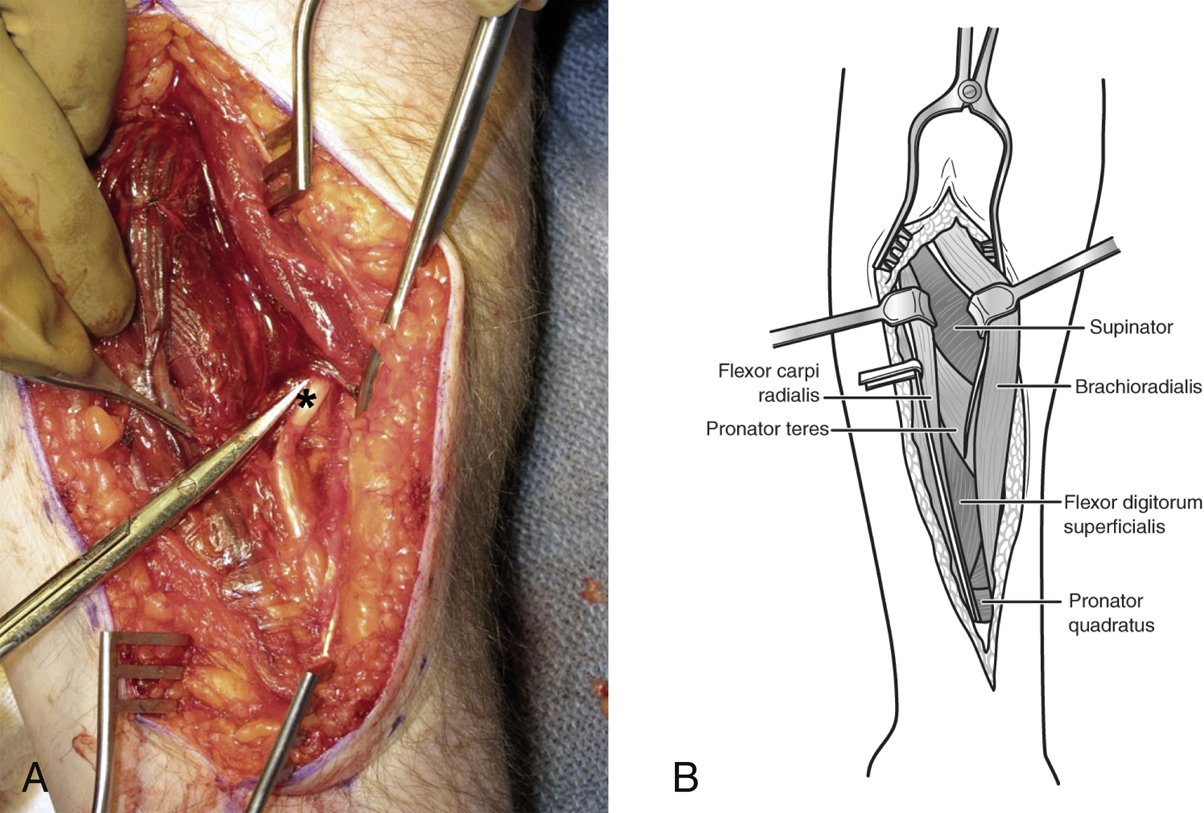
Figure 4Dissection in the midforearm for open reduction and internal fixation of a both-bone fracture. A, Intraoperative photograph shows the brachioradialis muscle retracted. The superficial radial nerve is denoted by the asterisk. B, Deep to the brachioradialis and the flexor carpi radialis are the supinator muscles, the pronator teres, the flexor digitorum superficialis, and, most distally, the pronator quadratus.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


