Open Reduction and Internal Fixation of Femoral Neck Fractures
Introduction
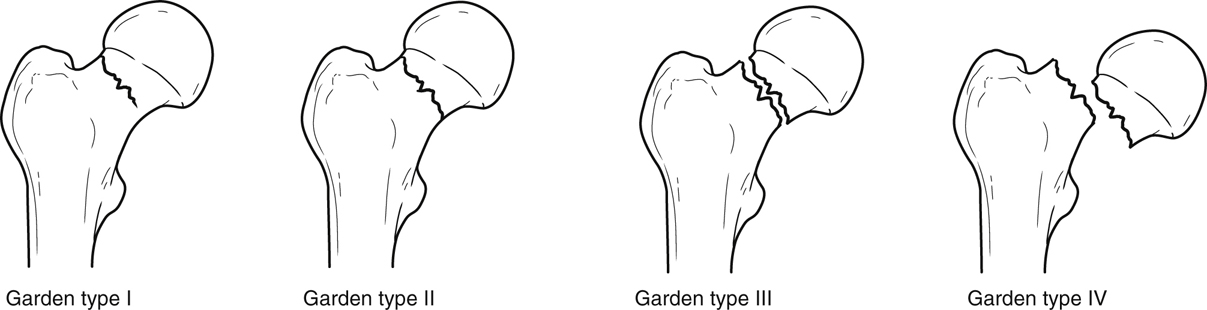
Figure 1Illustration shows the Garden classification of femoral neck fractures. Garden I: incomplete (most often valgus-impacted). Garden II: complete, nondisplaced. Garden III: complete, incompletely displaced. Garden IV: complete, completely displaced.
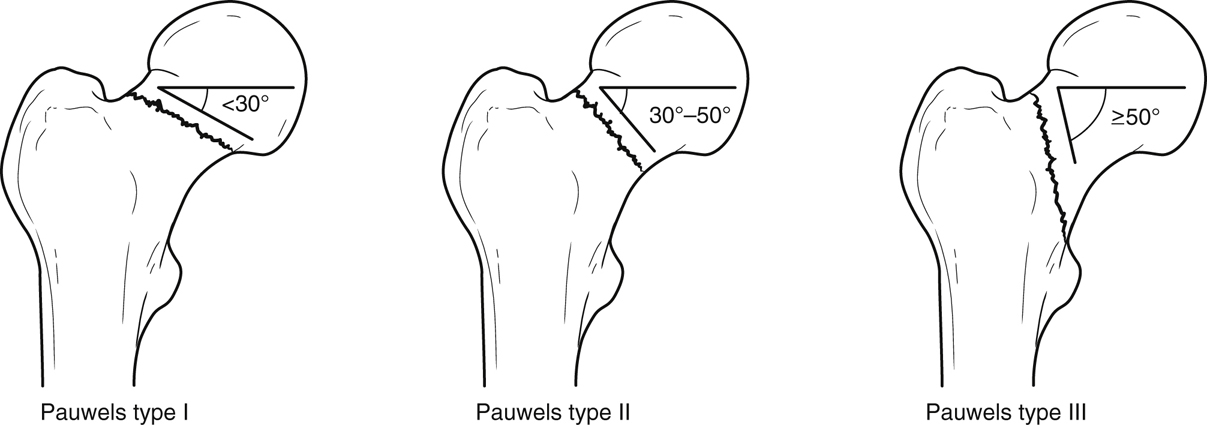
Figure 2Illustration depicts the Pauwels classification of femoral neck fractures. Type I: The angle subtended by the horizontal and the line of the fracture on an AP radiograph is less than 30°. Type II: The angle subtended by the horizontal and the line of the fracture on an AP radiograph is between 30° and 50°. Type III: The angle subtended by the horizontal and the line of the fracture is greater than or equal to 50°.
Femoral neck fractures occur from low-energy mechanisms (falls) in older people
More frequent in women than men (4:1)
In young patients, most commonly from high-energy mechanism
Can be intracapsular or extracapsular
Patient Selection
Manage femoral neck fractures surgically with anatomic reduction or arthroplasty; morbidity/mortality higher with nonsurgical management
Immobilization without fixation increases risk of pneumonia, pulmonary embolism, skin breakdown
Pain from unstable fracture increases narcotic requirement
Reserve nonsurgical management for frail patients and cases in which surgery is contraindicated
Consider percutaneous screw placement with local anesthetic in nonsurgical candidate with nondisplaced/incomplete fracture
For displaced fracture, consult pain control service to aid patients through acute phase
Preoperative Imaging
Plain Radiography
AP pelvis, AP/lateral hip
Gentle traction helps characterize fracture
CT and MRI
CT useful when open reduction and internal fixation (ORIF) planned and neck comminution present
Three-dimensional reconstruction helps characterize fracture
Procedure
Instruments/Equipment/Implants
Two Gelpi retractors
C-arm
Small, medium, and large pointed Weber tenaculum clamps
Two Freer elevators
Dental pick
Trocar-tipped terminally threaded Schanz pins (2.5 mm for femoral head fragment, 5.0 mm for distal trochanteric/femoral shaft fragment)
2.0-mm Kirschner wires (K-wires)
6.5- to 7.3-mm cannulated screws, or 130° blade plate/side plate (depends on fracture)
Bone graft if needed
Have minifragment set with 1.5- and 2.0-mm plates available
Surgical Technique
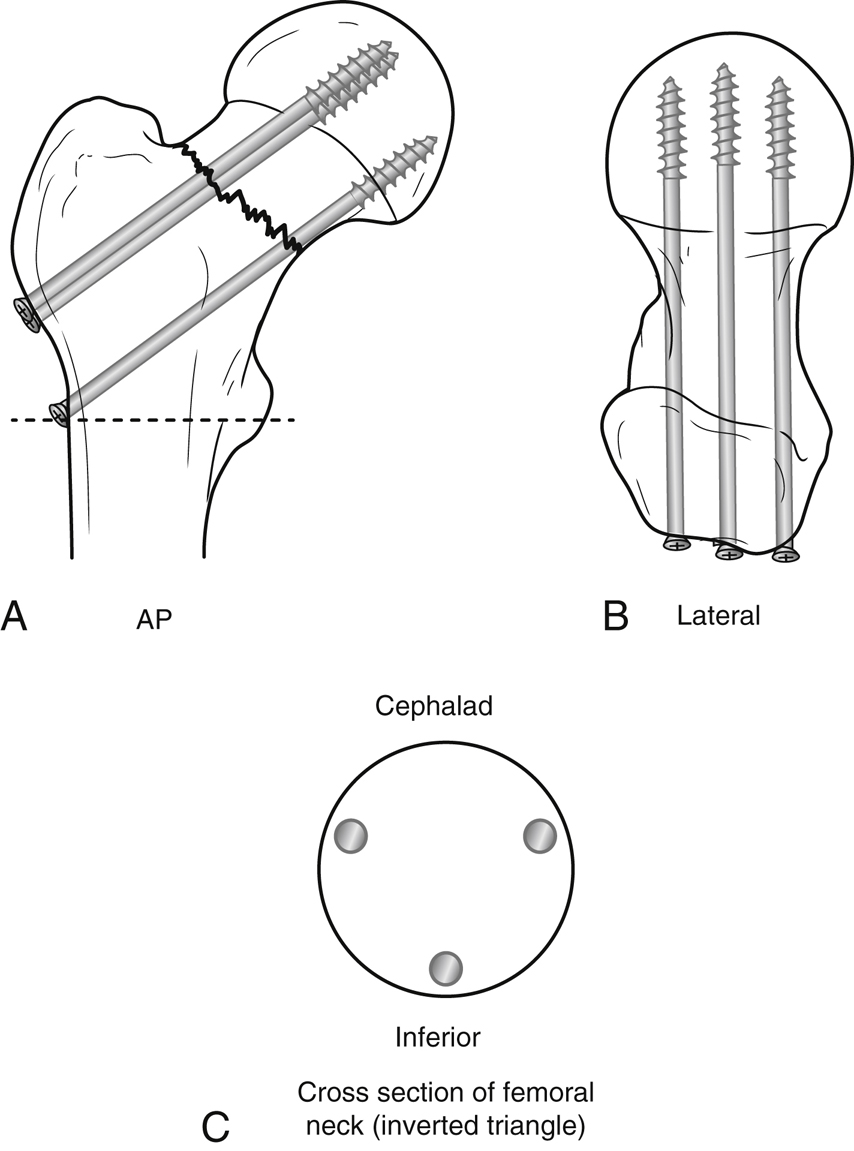
Figure 3Illustrations show correct screw placement for femoral neck fracture fixation using three screws, which usually is sufficient. The pattern of screw placement is important. A, The first screw is directed tangential to and contiguous with the calcar at the level of the fracture on the AP view. Starting screws below the level of the lesser trochanter (dashed line) should be avoided to minimize the likelihood of an iatrogenic subtrochanteric fracture. B, On the lateral view, the first screw is seen bisecting the head and neck. C, The spread between the screws should be maximized, as shown on the cross-sectional view of the neck.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


