Open Reduction and Internal Fixation of Distal Humerus Fractures
Patient Selection
Incidence of distal humerus fractures is 5.7 per 100,000 people per year
Treatment is generally surgical and can be challenging
AO/Orthopaedic Trauma Association classification
Type A—Nonarticular fractures
Type B—Partial articular fractures
Type C—Complete articular fractures
Goals of treatment—To obtain anatomic reduction with adequate stability to allow early range of motion (ROM)
Important to discuss loss of motion and possible transient ulnar nerve paresthesias with patient
Indications
Displaced fractures
Open or impending open fractures
Fractures with vascular injury
Ipsilateral upper extremity injury
Pathologic fractures
Contraindications
Poor health precluding tolerance of surgery
Active infection
Lack of appropriate soft-tissue coverage
Poor compliance
Extreme osteopenia
Nonsurgical treatment best for stable, nondisplaced fractures and patients with preexisting conditions creating nonfunctional limb
Preoperative Imaging
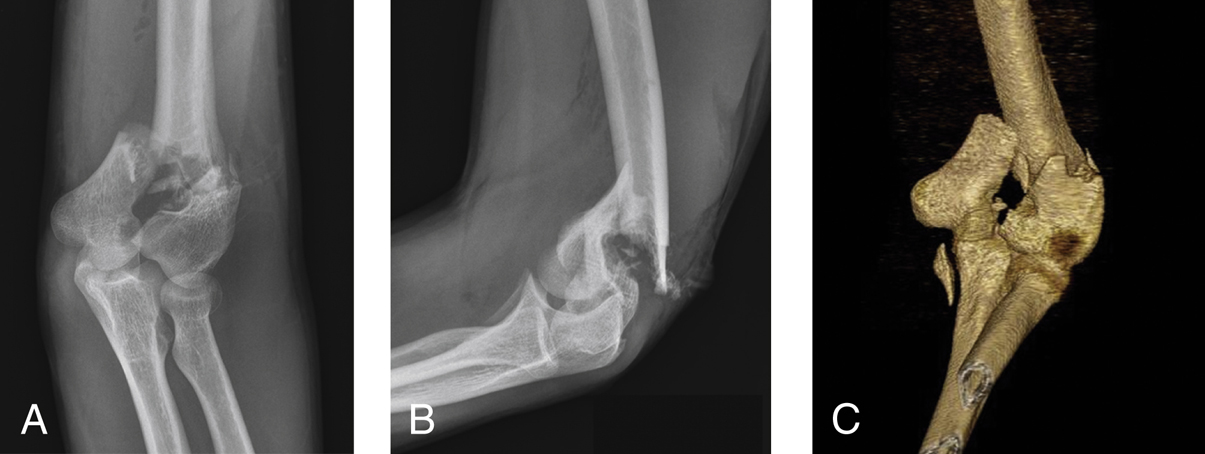
Figure 1AP (A) and lateral (B) preoperative radiographs demonstrate an intra-articular distal humerus fracture. Evidence of air also is seen, because this was an open fracture. C, CT reconstruction of the same injury shows a proximal ulnar fracture, which is not readily evident on the radiographs. This fracture was an avulsion of the ulnar insertion of the medial collateral ligament.
AP, lateral, and oblique radiographs of elbow
When indicated, shoulder and wrist radiographs
Traction radiographs and CT can be helpful (Figure 1)
Procedure
Room Setup/Patient Positioning

Figure 2Photograph shows a patient secured in the lateral decubitus position via a beanbag and safety strap, with the affected arm placed over a padded bolster. All bony prominences are padded appropriately.
Lateral decubitus position with arm over bolster provides excellent access (Figure 2)
Supine position for polytrauma patients
Pad all bony prominences
Position for ease of intraoperative imaging
Special Instruments/Equipment/Implants
Small-fragment plates, mini-fragment plates and screws, Herbert screws, Kirschner wires
Sterile tourniquet
Reduction clamps, osteotomes, oscillating saw
Wire set, bone-graft set
Mini C-arm fluoroscope
Surgical Technique
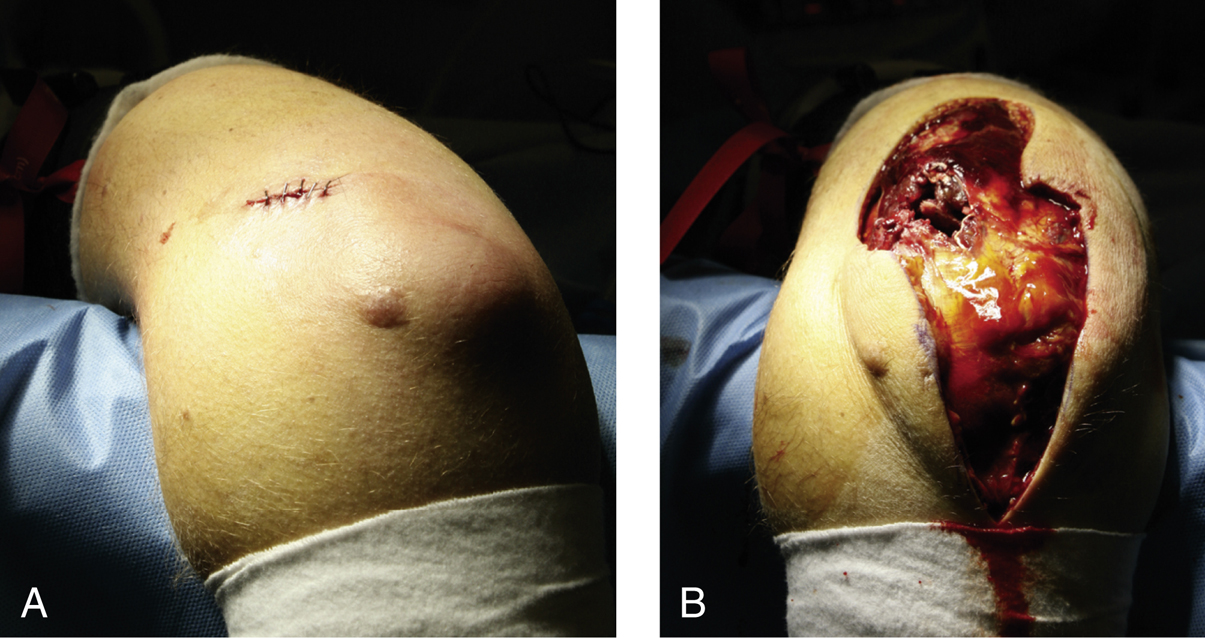
Figure 3Intraoperative photographs show the straight posterior approach for open reduction and internal fixation of a distal humerus fracture. The open fracture wound (A) was incorporated into the incision and the skin edges were excised (B). The large rent in the triceps and skin was created by the humeral shaft as it protruded at the time of injury. More than 90% of open wounds in this type of injury are posterior.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


