40 Open Reduction and Internal Fixation Lunate Dislocation via Combined Dorsal—Palmar Approach
Indications
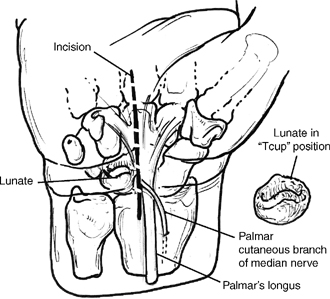
Technique
Related posts:
 Limited-Open Reduction and Percutaneous Pin Fixation with External Fixation of Distal Radius Fractures
Peripheral Tear of the Triangular Fibrocartilage Complex from the Ulna: Arthroscopic Repair
Fractures of the Ulnar Neck
Open Reduction and Internal Fixation of an Ulnar Styloid Fracture
Scapholunate Reconstruction with Dorsal Capsular Flap (Blatt Procedure)
Flexor Carpi Ulnaris Tenodesis Stabilization of the Resected Distal Ulna
Limited-Open Reduction and Percutaneous Pin Fixation with External Fixation of Distal Radius Fractures
Peripheral Tear of the Triangular Fibrocartilage Complex from the Ulna: Arthroscopic Repair
Fractures of the Ulnar Neck
Open Reduction and Internal Fixation of an Ulnar Styloid Fracture
Scapholunate Reconstruction with Dorsal Capsular Flap (Blatt Procedure)
Flexor Carpi Ulnaris Tenodesis Stabilization of the Resected Distal Ulna
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


