Oncologic Emergencies (Case 36: A Problem Set of Three Common Cases)
Minal Dhamankar MD and Zonera Ali MD
Case 1: A 77-year-old man with history of CLL presents with severe fatigue, nausea, and mild abdominal discomfort. He is found to have an elevated white count, splenomegaly, and bulky lymphadenopathy. He is admitted and started on chemotherapy. His basic metabolic panel is as follows: potassium 6.8 mEq/L, calcium 8.1 mg/dL, phosphate 7.0 mg/dL, LDH 28,900 U/L, uric acid 14.3 mg/dL, and creatinine 2.6 mg/dL (baseline creatinine before treatment was 1.0 mg/dL).
Differential Diagnosis
Renal Failure in Cancer Patients | ||
Tumor lysis syndrome (TLS) | Infiltration of kidneys by the underlying neoplastic process | Renal failure secondary to nephrotoxic chemotherapeutic agents |
Prerenal azotemia from volume depletion | Ureteral obstruction due to adenopathy | |
Differential Diagnosis
Low Back Pain and Leg Weakness in a Cancer Patient | |
Brain metastasis | Asthenia |
Lambert-Eaton myasthenic syndrome | Spinal cord compression (SCC) |
Case 3: A 55-year-old man with a history of acute myelogenous leukemia (AML) presents for a scheduled routine red blood cell (RBC) transfusion and reports fatigue. He is also receiving outpatient chemotherapy via a peripherally inserted central venous catheter (PICC). His temperature is 101°F, and blood pressure is 82/58 mm Hg with orthostatic changes. He is given 1 L of IV fluids and has routine laboratory samples drawn as he is transferred to the hospital. Upon admission, he is having rigors. His lab work shows a white blood cell count of 200 cells/µL and an absolute neutrophil count of 60 cells/µL.
Differential Diagnosis
Fever in a Cancer Patient | ||
Tumor fever | Neutropenic fever | Transfusion reaction |
Catheter-related sepsis | Drug fever | |
Speaking Intelligently
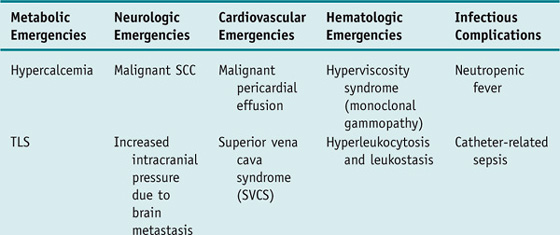
Patients with cancer are subject to developing a unique set of complications that require emergent evaluation and treatment. These oncologic emergencies can be broadly classified as those resulting from the disease itself and those resulting from therapy directed against the cancer; however, they can also be classified according to organ systems to facilitate recognition and management as follows (selected emergencies are discussed in more detail in the Clinical Entities section).
PATIENT CARE
Clinical Thinking
History
• New back pain that is not responding to routine pain medication, worsens when the patient lies down, or is associated with the development of leg weakness, urinary incontinence, and loss of sensory function warrants consideration of epidural SCC.
Physical Examination
Tests for Consideration
Laboratory studies include:
$11 | |
• Basic metabolic profile: Tumor lysis syndrome leads to a large number of metabolic derangements. | $12 |
$6 | |
$45 |
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


