24 Normal variants in children
Cases relevant to this chapter
Essential facts
1. In-toe gait becomes evident by age 2 years in 14–18% of infants and is usually secondary to persisting femoral anteversion.
2. Children with limb pains and ligament laxity may be diagnosed as having hypermobility syndrome, although most hypermobile children do not suffer such pains.
3. Bow legs (genu vara) are normal till age 2, after which knock-knees (genu valga) become the norm.
4. Painless flat feet that develop normal arches when the child stands on tiptoe require no treatment other than reassurance.
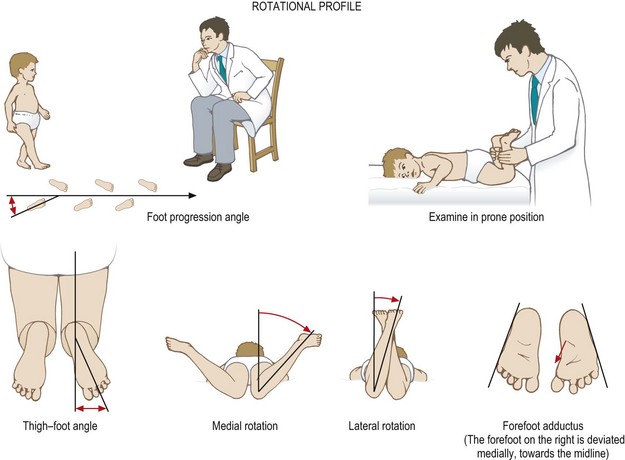
Most books cover diseases, yet normal variants and normal developmental stages cause considerable anxiety to parents and doctors. Normal children have a rotational profile to their gait, as shown in Figure 24.1.
Bow legs and knock-knees
All children are bow-legged (genu vara) until age 2 when they become knock-kneed (genu valga). Genu vara appears greater in a child who in-toes. Genu valga is maximal between ages 3 and 4 years, and may be more marked in children who have ligament laxity or are overweight. The adult alignment of slight valgus is usually achieved by age 9 (Fig. 24.2). Bow legs beyond age  years or knock-knees before 18 months are probably pathological, in which case rickets or an inherited skeletal dysplasia that can cause either genu vara or valga should be excluded. Persisting bow legs in a heavy early walker may be due to Blount’s disease (medial growth delay or arrest of the proximal tibial physis). This condition is more common in African Caribbeans. If detected early, it can readily be corrected surgically by a medial periosteal release. If detected late, complex osteotomies are required to correct this tri-planar deformity.
years or knock-knees before 18 months are probably pathological, in which case rickets or an inherited skeletal dysplasia that can cause either genu vara or valga should be excluded. Persisting bow legs in a heavy early walker may be due to Blount’s disease (medial growth delay or arrest of the proximal tibial physis). This condition is more common in African Caribbeans. If detected early, it can readily be corrected surgically by a medial periosteal release. If detected late, complex osteotomies are required to correct this tri-planar deformity.
< div class='tao-gold-member'>

Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


