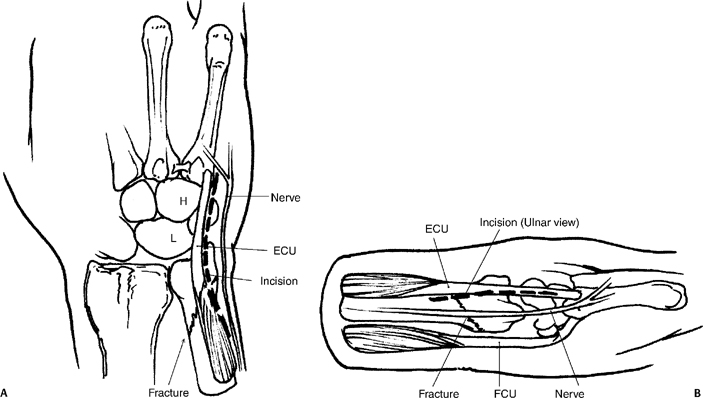
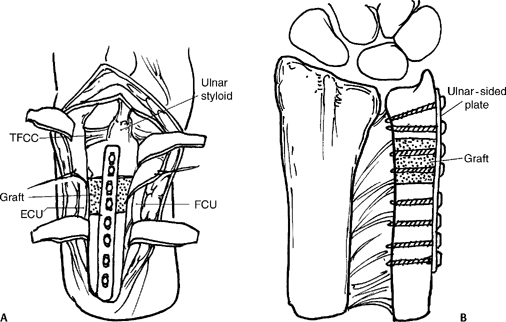
15 Nonunion of an Ulnar Neck Fracture A significant bone defect is typically present after removing the sclerotic margins of the bone and the previously placed hardware. To avoid excessively shortening the ulna it is usually necessary to place intercalary, tricortical iliac crest bone graft. To re-create the appropriate ulnar variance take PA projection of the contralateral wrist with the forearm pronated. Figure 15-1
Indications
Pitfall
Pearl
Technique
Related posts:
 Intra-articular Fractures of the Distal Radius Treated with Dorsal Plate
Intra-articular Fractures of the Distal Radius Treated with Dorsal Plate
 Resect Ulnar Styloid Fracture with Repair of Triangular Fibrocartilage Complex
Resect Ulnar Styloid Fracture with Repair of Triangular Fibrocartilage Complex
 Percutaneous Screw Fixation of Scaphoid Fractures
Percutaneous Screw Fixation of Scaphoid Fractures
 Flexor Carpi Radialis Tendon Stabilization of the Scapholunate Joint (Brunelli Procedure)
Flexor Carpi Radialis Tendon Stabilization of the Scapholunate Joint (Brunelli Procedure)
 Closed Reduction and Internal Fixation of Bennett’s or Rolando’s Fractures
Closed Reduction and Internal Fixation of Bennett’s or Rolando’s Fractures
 Capitate Shortening with Capitohamate Fusion
Capitate Shortening with Capitohamate Fusion
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


