TABLE 33-1 SEDDON’S CLASSIFICATION OF NERVE INJURY | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
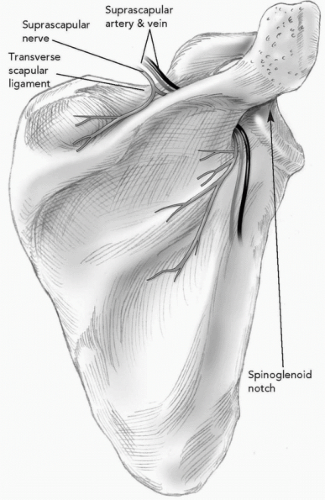 Figure 33-1 Suprascapular nerve passes below the transverse scapular ligament and around lateral margin of the scapular spine (spinoglenoid notch). |
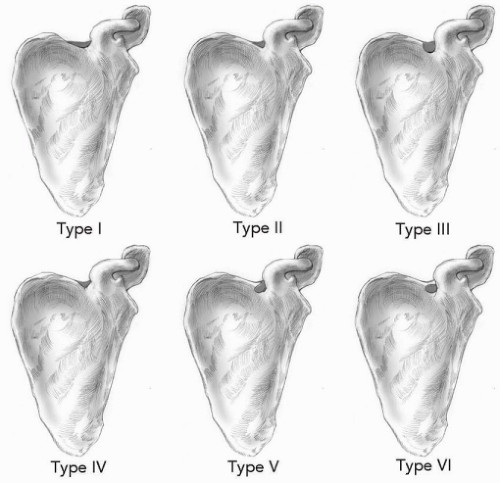 Figure 33-2 Classification of suprascapular notch morphology. In type I, the entire superior border of the scapula shows a depression (8% of specimens). In type II, there is a wide, blunted, V-shaped notch (31%). In type III, the notch is symmetrical and U-shaped (48%). In type IV, there is a very small V-shaped notch (3%). Type V is similar to type III but with partial ossification of the medial portion of the transverse scapular ligament (6%). In tye VI, the transverse scapular ligament is completely ossified, resulting in a foramen of variable size (4%). (Adapted from Rengachary SS, Burr D, Lucas S, et al. Suprascapular entrapment neuropathy: a clinical, anatomical, and comprehensive study. Part 2: anatomical study. Neurosurgery 1979;5:447.) |
TABLE 33-2 CAUSE OF SUPRASCAPULAR NEUROPATHY | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
|
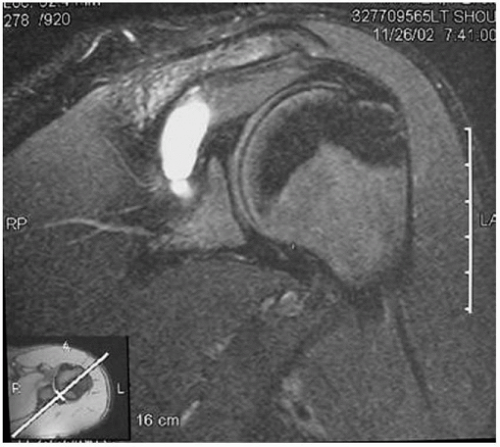 Figure 33-3 Magnetic resonance imaging (MRI) of glenohumeral cyst emanating from the posterior-superior capsularlabrum junction and compressing the suprascapular nerve before innervation of the infraspinatus muscle. |
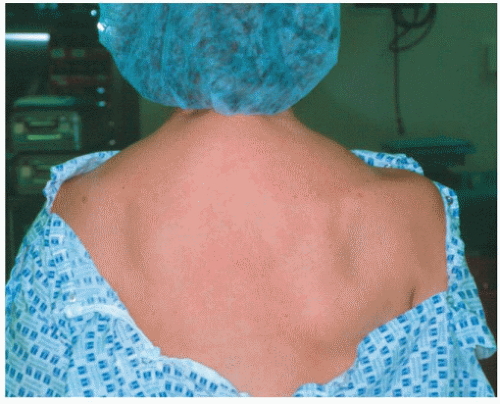 Figure 33-4 A 30-year-old woman with right suprascapular notch neuropathy and diffuse atrophy of both the supraspinatus and infraspinatus muscles. |
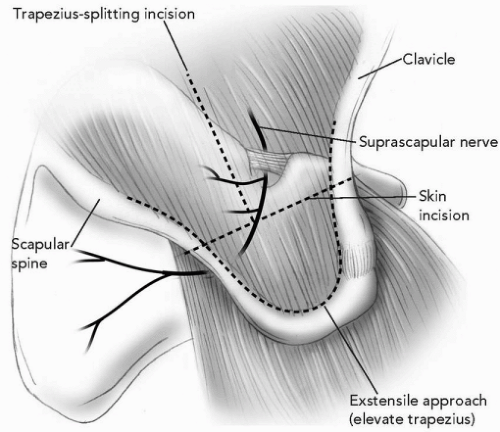 Figure 33-5 Superior trapezius-splitting approach for decompression of suprascapular notch neuropathy. |
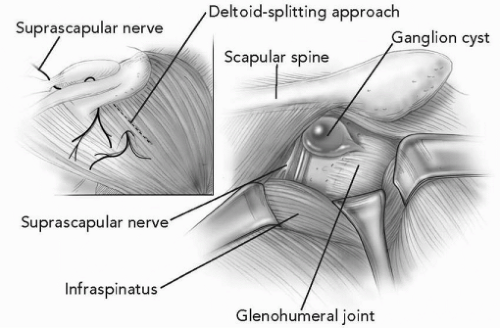 Figure 33-6 Posterior approach to the shoulder for isolation of the suprascapular nerve and excision of glenohumeral cyst. |
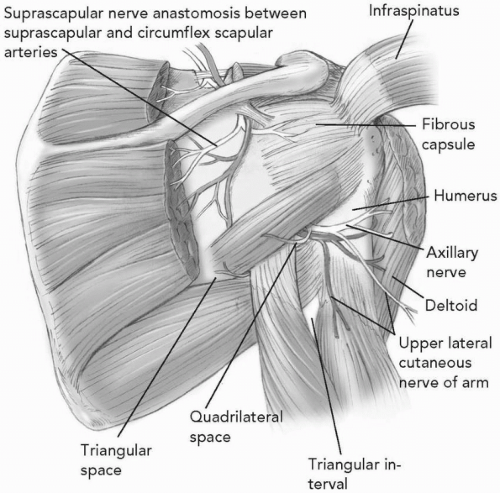 Figure 33-7 Posterior view of quadrilateral space with axillary nerve and posterior humeral circumflex artery. |
TABLE 33-3 CAUSE OF AXILLARY NEUROPATHY | ||||||||
|---|---|---|---|---|---|---|---|---|
|
Related posts:
 Three-Part Fractures: Open Reduction and Internal Fixation, or Arthroplasty?
Anterior Superior Rotator Cuff Tears: Repairable and Irreparable Tears
Arthroscopic Repair of Rotator Cuff Tears
Massive Tears of the Posterosuperior Rotator Cuff
Acute Fractures, Malunions, and Nonunions of the Clavicle
Arthrodesis and Other Salvage Procedures: When Arthroplasty Is Not Indicated
Three-Part Fractures: Open Reduction and Internal Fixation, or Arthroplasty?
Anterior Superior Rotator Cuff Tears: Repairable and Irreparable Tears
Arthroscopic Repair of Rotator Cuff Tears
Massive Tears of the Posterosuperior Rotator Cuff
Acute Fractures, Malunions, and Nonunions of the Clavicle
Arthrodesis and Other Salvage Procedures: When Arthroplasty Is Not Indicated
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


