9
Needling Techniques and Selection
From the Ling Shu: “The importance of the de qi lies in the ability to feel the arrival of qi. The judgment of therapeutic effect depends on it. In the process of acupuncture, first watch for the approaching of qi to the point of de qi. If however, nothing arrives at the end of treatment, healing of disease is not to be expected.” – Zhen Jiu Da Cheng
“You can’t expect both ends of a sugar cane to be sweet.” – Chinese Proverb
Anatomy of an Acupoint
Professor Dr. Hartmut Heine, from the Institute für Antihomotoxikologie und Grundregulation in Baden-Baden, Germany, discovered the anatomical basis for acupuncture points (acupoints) in 1987 at the University of Witten, Herdecke, Germany. In the superficial body fascia, the corpus superficialis, there are collagenous layers separating the connective tissue of the skin and the muscles. The fascia corpus superficialis covers the entire body except the head, fingers, and toes. Near the acupuncture points, the fascia corpus superficialis is penetrated by a nerve-vessel bundle covered loosely with connective tissue. This nerve-vessel bundle is made up of arteriole capillaries, veins, venules, unmyelinated nerve fibers, and myelinated nerves with lymphatic vessels just above the superficial fascia. The acupoint is described as a vertical column, one could say a chimney, of loose connective tissue that is surrounded by the thick, dense connective tissue of the skin.1 This perforation is present in the form of a laceration or a round opening. For this reason, there is a decrease in electrical resistance near the acupuncture point. Even in areas of the body where there is no superficial body fascia, such as the head, fingers, and toes, there are acupuncture points that can be demonstrated. These points are quite often sensitive. In the temporal region there is superficial temporal fascia, fatty tissue with veins and nerves over a deep sheath of temporal fascia. In other areas, going from superficial to deep, there is the superficial sheath of the temporal fascia followed by a deep sheath of temporal fascia, followed by the temporal artery with nerves. It is in this subcutaneous area below the deep sheath of the temporal fascia, and superior to the periosteum of the temporal bone, that one will place the acupuncture needle tip for effective YNSA treatment. This area of connective tissue houses nerves and vessels. It is from the selective bioelectrical stimulation with the acupuncture needle on these biocircuits of tissues, nerves, and vessels that physiological and biochemical changes are initiated.
Reichmamis in 1997 demonstrated electrical correlates of acupuncture points and documented the low resistance pathways for the flow of electricity along the acupuncture channels.2 Yoshio Manaka in 1995 proposed the X-Signal System Theory. The X-Signal System represents a permanent regulatory system that is different from the classical nerves or hormonal system. This primitive sensory system is present in single-cell animals that did not have nerves per se but nevertheless reacted to external stimuli. The energy fields of the body and the perineural system, along with the living matrix, are some of the substrates through which the X-Signal System exerts its effects on the cells and tissues. Stimulation of the channel and its branches extends to every part of the body including the surfaces and interiors of each individual cell and organelle. Manaka theorized that through this primitive system one is able to influence all of the cells in the body through acupuncture. It is because the molecular web of the body is more than a mechanical anatomical structure; it is a continuous vibratory network and as such presents possibilities of great significance.3 See also the discussion of the paper by Kenneth Pienta and Donald Coffrey on pages 46–47.
The Needle
A sterile, filiform non-cutting needle is the needle for performing acupuncture. It is generally made from stainless steel wire that is sharpened at one end. At the opposite end is a handle composed of thin, double-wound copper wire, stainless steel, silver, or molded piece of plastic. The needle has a point, which is described as bullet shaped, where the needle is used to push aside the horny plates of the epidermis, as opposed to cutting through the skin like a hypodermic or cutting (suturing) needle. The body of the needle is the part that is placed within the skin and scalp. At the end of the handle is a small tail where the copper or silver metal is wound in a double loop. Sterilized stainless steel needles are the best because of flexibility, strength, and resistance to oxidation.4 The copper wire handle is preferred because it offers more electrical potential based on the physics of the two different metals—copper attached to stainless steel. Stainless steel, silver, or gold handles are energetically preferred over plastic.
Physics of the Needle
The physics of the copper-wound acupuncture needle has more than just electrical potential effects between the low resistance acupoint, the stainless needle conduction, and the difference between the copper and stainless steel electro-scalar and magnetic vector potentials. Those two gradient potentials are usually enough to have a bioelectrical effect, as demonstrated with the ordinary stainless steel needles with either an annealed stainless steel or plastic handle, but the copper-wound needles possess other physical influences as demonstrated through the Aharonov-Bohm effect, a cornerstone of quantum mechanics.5
In classical physics, waves can interfere with each other. When two waves of the same frequency are in phase, their amplitudes add together to create larger waves; this is called constructive interference. When their waves are exactly out of phase, their amplitudes subtract and they can partially or completely cancel or destroy each other; this is called destructive interference. In nature, these interacting waves have a mix of frequency phases and therefore add and subtract in a very complex manner.
Wittaker and Tesla in 1904 generated potential waves and called them “non-hertzian waves.”2 When a magnetic field induces a current flow in a conductor, such as an acupuncture needle, it is actually the potential component of the field and not the field itself that underlies the effect. The potentials are of two types: scalar and magnetic vectors. Aharonov and Bohm in 1959 showed these potentials to have a physical reality.6 A magnetic vector potential occurs when electrons pass through the force field region around a coil, as in a coiled copper-wound needle. Though there was no electricity, nevertheless these electrons undergo a phase change indicating that some nonelectric, nonmagnetic physical entity must be acting on it. Thus, the entity is called a magnetic vector potential.
Further research showed the existence of electric scalar potential in a region where no electric field existed. Thus, in destructive interference, where two electrical potentials cancel each other, electrostatic scalar potentials and magnetic vector potentials still remain. In essence, the energy and information contained in the original waves are not destroyed by interference.
Various kinds of coil designs enable the vectors of the electric and magnetic fields to destructively interfere or cancel each other out. The standard coil emits electric and magnetic fields in the space around it. The bifilar coil has the electric and magnetic fields cancelling each other out, thus producing electric scalar and magnetic vector fields. This bifilar coil is similar to the copper coil on copperwound acupuncture needles, which produces electric scalar and magnetic vector waves. According to Jacob and Rein, scalar waves appear to interact at atomic nuclei rather than with electrons. These interactions are described by quantum chromodynamics. Oschman states that scalar waves appear to be intimately involved in healing and are probably emitted by living systems.2
Needle Selection
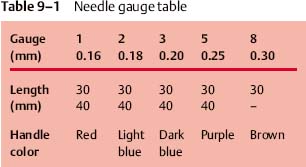
Acupuncture needles used in YNSA are typically gauge 2, 3, 5, and, rarely, 8, see Table 9–1. The typical length is either 30 mm or 40 mm for gauge 2, 3, and 5; for gauge 8, 30 mm is sufficient. Gauge 5 followed by gauge 2 are the most commonly used in the author’s YNSA experience. Gauge 8 0.30 mm needles are only used on very tightly restricted calcifications identified subcutaneously in the scalp or where a gauge 5 needle is not able to separate this calcification. A thin needle provides a less potent stimulus than a thicker needle but causes less pain. Gauge 2 is preferred for YNSA points on the forehead.
Presterilized disposable needles with tubes are ideally used in YNSA. As one places the finger of one hand over the point, one can with the other hand then slide the needle in the tube over the point, thus making sure one is exactly on the point with greater accuracy by using the tube. The use of the tube aids in getting the correct prescribed depth for initial needle insertion, presenting the needle in a vertical position, ready to be adjusted to the correct angle as needed, in as sterile and clean a manner as possible through hair.
The constant controversy of what is the best (the thinnest, pain-free, but powerful) needle for one to use is the acupuncturist’s elusive quest. The goal of the YNSA physician acupuncturist is to place the needle as painlessly as possible in the subcutaneous tissue to bioelectrically stimulate the body, thereby alleviating pain and restoring harmony and physiological balance. Often there are subcutaneous calcifications especially at the Basic point lines; for example, A-1–7, C-1, C-2, that require a stiff needle to be used to help separate the partially calcified subcutaneous tissue. However, using the thinnest needle offers the least amount of pain to the patient. Taking that into consideration, identifying the thinnest possible needle that does not bend and yet has a powerful effect is still the challenge.
Patient Position
The most common patient position is seated; occasionally they are supine or prone. For patients who suffer from a history of needle shock or fainting, a supine posture is recommended if YNSA is used at all, otherwise the patient is seated facing the physician.
Clean Needle Technique
Sterilizing the scalp is not done. Utilizing sterile single use disposable needles (preferably with an insertion tube) on a clean field is sufficient. Sterilizing the scalp can only be done with standard sterile procedures, which include shaving the head, followed by painting the scalp with 2% Iodine that may or may not be removed by isopropyl alcohol, and then properly draping the head to provide a sterile field. This, of course, is not done in YNSA.
In YNSA technique, when placing a sterile needle in the scalp, passing through the hair to get to the scalp, and keeping the needle sterile with or without a sterile tube is, for all intents and purposes, impossible. Simply using sterile needles on clean (recently washed) scalp and hair is acceptable; however, clean needle placement is recommended. “Clean needle technique” is defined by Jenny Belluomini as:
1. Wash hands before and after patient contact.
2. Swab the insertion site with alcoholized sterile gauze or sterile cotton ball. (Caution—Hair dyes and coloring may be altered with alcohol. Consult with patient before using.)
3. Keep needle shaft sterile (using a sterile tube) until it is inserted into the skin.
4. Use gloves if coming in contact with body fluids, which is unlikely in YNSA.7






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


