Needle Aponeurotomy
Introduction
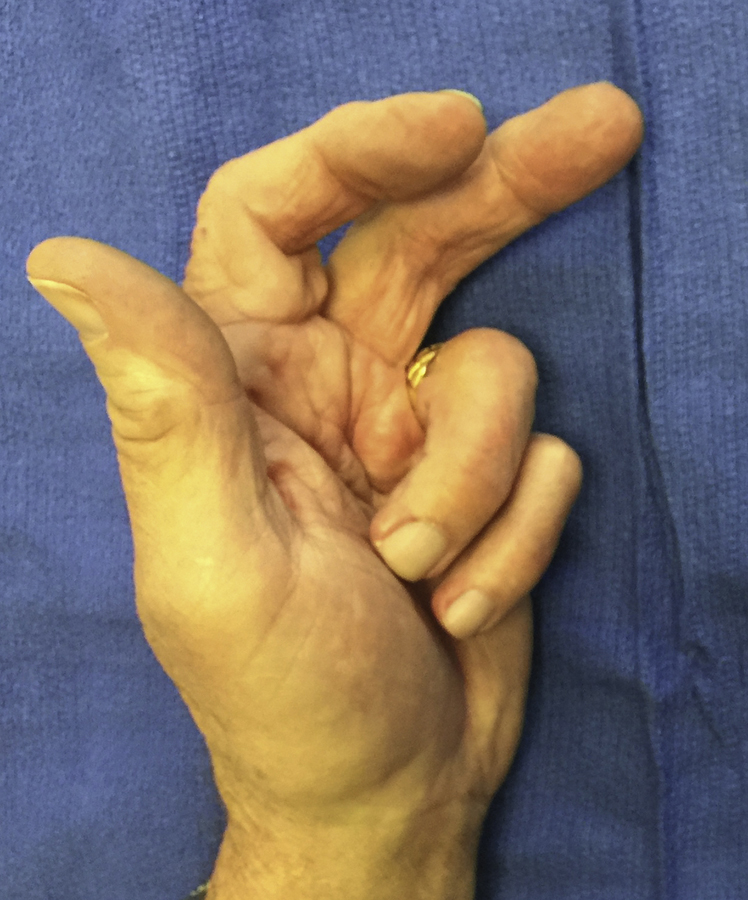
Figure 1Photograph of severe untreated Dupuytren disease.

Figure 2Photograph of mild Dupuytren disease.

Figure 3Photograph of complete correction of mild Dupuytren disease with needle aponeurotomy (NA).
Dupuytren disease is a benign fibromatosis of the fascia of the hand and fingers
Starts as nodule or palpable mass and enlarges and leads to development of pathologic cords which thicken and contract (Figures 1through 3)
Most commonly affected digits are the ring and little finger (50% to 60%)
Patient Selection
Indications
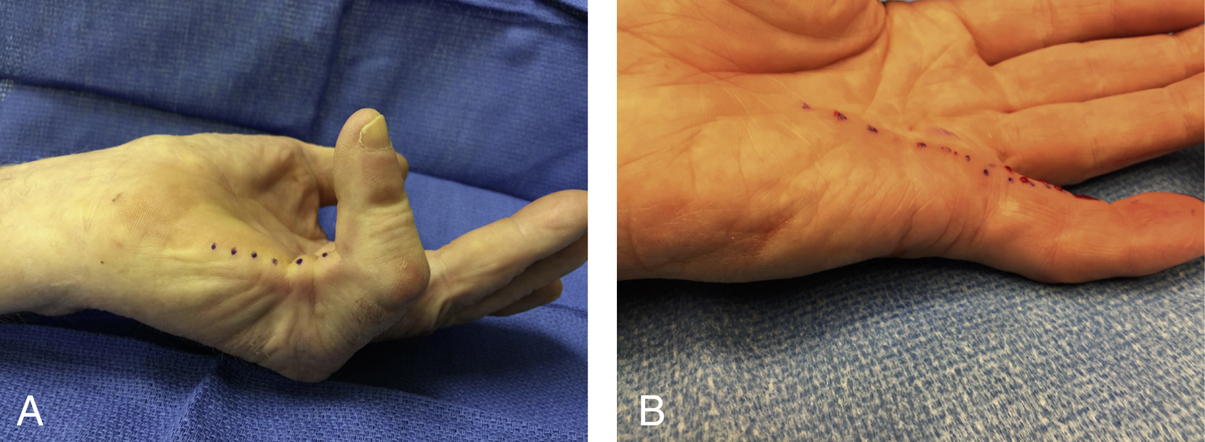
Figure 4Photographs showing that the area of maximum bowstringing is the best location for needle aponeurotomy (NA) portals. A, Before. B, After.
Palpable cords causing contracture (Figure 4)
Contraindications

Figure 5Photograph shows that needle aponeurotomy (NA) can be performed as long as a palpable cord is present and the contracture is not just due to scar.
Contracted skin, skin grafts, and scar tissue from prior fasciectomy (Figure 5)
Contractures secondary to spasticity or ulnar nerve palsy
Surgical Anatomy

Figure 6Illustration of anatomy of pathologic cords. 0 = central cord; 1 = pretendinous cord; 2 = distal commissural cord; 3 = abductor digiti minimi cord; 4 = lateral cord; 5 = natatory cord; 6 = proximal commissural cord; 7 = retrovascular cord; 8 = spiral cord; 9 = thumb pretendinous cord.
(Redrawn from an illustration provided courtesy of Charles Eaton, MD.)
Pretendinous cord—originates from pretendinous band, begins proximal to the proximal finger crease, contracts the MP joint of fingers or thumb
Central cord—located midline between neurovascular bundles and distal to the proximal finger crease, is a continuation of the pretendinous cord, contracts the PIP joint
Lateral cord—composed of diseased lateral digital fascia, located superficial to neurovascular bundle, contracts PIP joint
Retrovascular cord—located deep to neurovascular bundle, can contract both the PIP and DIP joints
Natatory cord—contracts the second, third, and fourth web spaces
Commissural cords (proximal and distal)—contracts the first web space, may be rope-like in consistency
Abductor digiti minimi cord—contracts the little finger MP and PIP joints. Can displace the neurovascular bundle in a volar, midline, and distal direction
Spiral cord—contracts PIP joint—usually a combination of pretendinous cord, diseased lateral digital fascia, and Grayson’s ligament. Can displace neurovascular bundle in a volar, midline, and distal direction (Figure 6)
Preoperative Imaging
No special imaging necessary
Plain radiographs useful to evaluate articular surfaces for long-standing severe contractures
Radiographs required in setting of old injury or dislocation
Procedure
Room Setup/Patient Positioning
Performed usually in outpatient treatment room under local anesthesia
For patients with low pain tolerance, sedation can be used in surgery center or hospital setting; patient must remain responsive to stimuli and communication
Recumbent or sitting position
No tourniquet
No prophylactic antibiotics
Special Instruments/Equipment
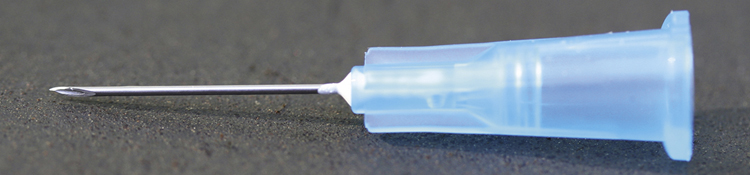
Figure 7Photograph of a short 25-gauge, 16-mm (5/8-inch) needle with which needle aponeurotomy is performed.
5 mL syringe filled with 3 mL lidocaine 1% plan and 1 mL methylprednisolone acetate injectable suspension 40 mg
Short 25-gauge needle, 16 mm (5/8 inch) length needles (Figure 7)
18-gauge, 40 mm (1.5 inch) needle can be bent to 90° for subcision
Clamp/needle holder
Surgical Technique
 | Video 50.1 Treatment of Dupuytren Disease With Needle Aponeurotomy. Gary M. Pess, MD (2 min 30 s) |
 | Video 50.2 Treatment of Dupuytren Disease of PIP Joint With Needle Aponeurotomy. Gary M. Pess, MD (2 min 25 s) |
Preoperative Planning
Abnormal cords are identified by palpation and marked with surgical marker
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


