Nail Matrix Repair, Reconstruction, and Ablation
Reuben A. Bueno Jr.
Elvin G. Zook
DEFINITION
Injury to the nail usually occurs by traumatic setting. Because of its location at the distal end of the digits, the perionychium is the most frequently injured part of the hand.9
Restoration of normal nail appearance and function is best achieved by acute repair of the nail matrix.
Reconstructive techniques may be used to provide a more normal-appearing nail.
Excision of benign and malignant tumors involving the nail bed matrix may require techniques of nail bed repair and reconstruction also used for trauma.
Optimal treatment depends on thorough understanding of the components of the perionychium—skin, sterile matrix, germinal matrix, eponychial fold, and distal phalanx—and their anatomic relationship with each other.
ANATOMY
The nail serves multiple functions: protecting the fingertip, regulating peripheral circulation, and contributing to sensory feedback of the fingertip.9,10
The perionychium includes the nail plate, nail bed, hyponychium, eponychium and fold, and paronychium (FIG 1).
The proximal portion of the nail matrix (approximately one-fourth of the nail length) is the germinal matrix and the distal three-fourths is the sterile matrix. The germinal matrix produces about 90% of the nail, whereas the sterile matrix produces the remaining 10% of the nail and produces the cells on the undersurface of the nail responsible for nail adherence.
The hyponychium is the skin distal to the nail bed, the paronychium is the skin on each side of the nail, and the eponychium is the skin over the nail fold.
The nail bed is adherent to the periosteum of the distal phalanx.
PATHOGENESIS
The main causes of nail deformity are trauma and tumor.
The middle finger is the most commonly injured finger because of its length.13
Inadequate treatment in the acute setting often leads to a nail deformity.
There is an associated distal phalanx fracture in 50% of nail bed injuries. This type of injury should be considered an open fracture and treated as such with irrigation and débridement, reduction of the fracture and fixation if necessary, and repair of the nail bed (FIG 2).1,4
Scarring can lead to a split nail deformity.
Absence of nail matrix can lead to detachment of the nail.
Lack of support from the distal phalanx leads to the hook nail deformity.
Benign tumors (glomus tumor, distal interphalangeal joint ganglion) and malignant tumors (squamous cell carcinoma, melanoma) can affect nail appearance.
NATURAL HISTORY
Repair in the acute injury period provides the best chance for normal appearance of the nail.
The nail plate grows at about 0.1 mm per day or 2 to 3 mm per month. When the nail plate is removed for nail bed repair, new nail growth is delayed for 3 to 4 weeks.9
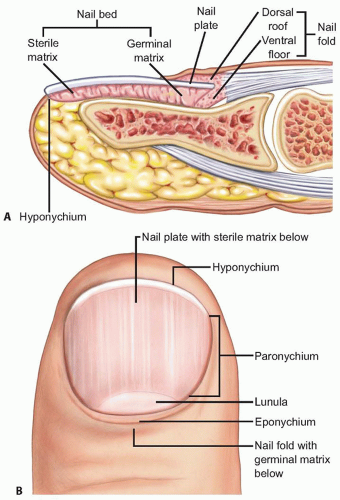
FIG 1 • A,B. The perionychium and its associated structures.
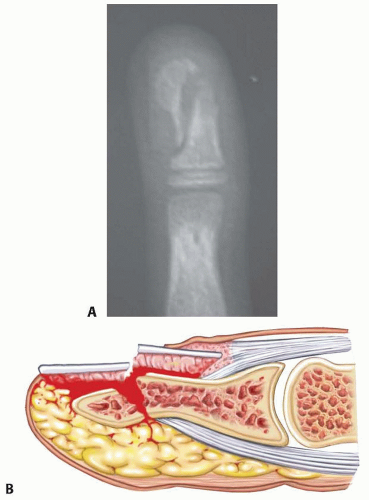
FIG 2 • A. Radiograph showing distal phalanx fracture associated with a nail bed crush injury. B. Nail bed injury with concomitant distal phalanx fracture. With a break in the periosteum, there is communication of the distal phalanx with the outside environment. There is a risk for osteomyelitis if not treated appropriately.
If placed back on after repair, the old nail will remain adherent for 1 to 3 months and then fall off as a new nail pushes it off.12
PATIENT HISTORY AND PHYSICAL FINDINGS
In the acute setting, the status of the entire fingertip must be assessed: quality of the skin, presence of a subungual hematoma, quality of the nail matrix, capillary refill, sensory function, flexion and extension at the distal interphalangeal joint, and presence of a distal phalanx fracture.
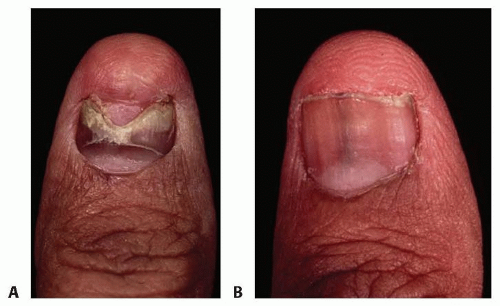
FIG 3 • A. Nail appearance at 3 months after repair. Patients should be aware of the heaped-up appearance as the nail grows distally. B. Nail appearance at 1 year after repair.
Features of acute nail bed injury
Subungual hematoma (FIG 4A,B): bleeding beneath the nail from laceration of the nail bed
Pain secondary to pressure in the space between the nail plate and the nail bed
Treated with evacuation of hematoma by trephination
Laceration of nail bed (FIG 4C,D)
Mechanism of injury usually is crush.
Concomitant injury to fingertip skin or distal phalanx fracture may be present.
Nail lacerations can be described in one of four ways: simple laceration, stellate laceration, severe crush, and avulsion.
Repair of nail bed laceration and Kirschner wire fixation of distal phalanx fracture if unstable
Nail bed avulsion (FIG 4E)
Quality of avulsed nail matrix and size of defect will determine treatment.
Treatment options include returning avulsed piece back into the defect or harvesting a split nail graft from the adjacent matrix or from the great toe. (A skin graft will prevent new grooving nail to adhere.)
Posttraumatic nail deformities
Nail nonadherence or split nail (FIG 4F)
Usually due to injury to the sterile matrix, which produces the cells responsible for adherence
Excision of scar and primary closure or nail matrix reconstruction with a split graft from the great toe
Hook nail deformity (FIG 4G)
Due to excessive tension at junction of nail bed and hyponychial skin and loss of support of distal phalanx
Revision amputation or reconstruction of nail bed and bone graft to the distal tip of the distal phalanx
Nail remnant (FIG 4H)
Due to presence of residual germinal matrix not completely ablated at the time of initial repair or revision amputation
Complete nail matrix ablation or revision amputation
Pincer nail deformity (FIG 4I): characterized by excessive transverse curvature of the nail and progressive pinching off of the distal fingertip, causing pain and abnormal appearance
Partial or complete nail ablation
Reconstruction of nail bed with elevation of the lateral nail bed using dermal graft or AlloDerm
IMAGING AND OTHER DIAGNOSTIC STUDIES
Anteroposterior (AP) and lateral radiographs of the distal phalanx are recommended to rule out a fracture.
Depending on the level of injury, the following fractures are seen: distal tuft fracture, comminuted fracture, and a transverse or oblique fracture of the midshaft.
Intra-articular fractures at the distal interphalangeal joint are rare with an associated nail bed injury.
DIFFERENTIAL DIAGNOSIS
Trauma
Benign tumor
Glomus tumor
Distal interphalangeal joint ganglion cyst
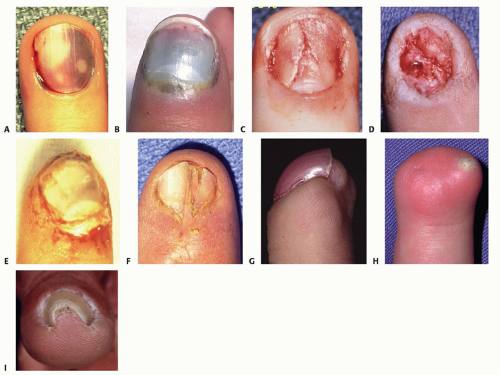
FIG 4 • Nail deformities. A,B. Subungual hematoma. C,D. Laceration of nail bed. E. Nail bed avulsion out of eponychial fold. F. Split nail deformity. G. Hook nail deformity. H. Nail remnant. I. Pincer nail deformity.
Malignant tumor
Squamous cell carcinoma
Melanoma
NONOPERATIVE MANAGEMENT
Left untreated, traumatic injury to the nail matrix may result in an abnormal appearance and shape of the nail.
SURGICAL MANAGEMENT
Repair in the acute period increases the chance of a normal-appearing nail.Related posts:
 Anatomy and Surgical Approaches of the Forearm, Wrist, and Hand
Anatomy and Surgical Approaches of the Forearm, Wrist, and Hand
 Arthroscopic Treatment of Chondral Injuries and Osteochondritis Dissecans
Arthroscopic Treatment of Chondral Injuries and Osteochondritis Dissecans
 Fragment-Specific Fixation of Distal Radius Fractures
Fragment-Specific Fixation of Distal Radius Fractures
 Arthroscopic and Open Triangular Fibrocartilage Complex Repair
Arthroscopic and Open Triangular Fibrocartilage Complex Repair
 Carpal Tunnel Release: Endoscopic, Open, and Revision
Carpal Tunnel Release: Endoscopic, Open, and Revision
 Surgical Treatment of Acute and Chronic Paronychia and Felons
Surgical Treatment of Acute and Chronic Paronychia and Felons

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


