Chapter 29 Miscellaneous cases in adulthood
Case 29.1
Case 29.2
| Disorder | Aetiology | Clinical features |
|---|---|---|
| Phimosis | • It may also be due to scarring following the trauma of forcible retraction of the prepuce or from chronic balanitis | • In physiological phimosis, the prepuce is seen to balloon during micturition, and the urinary stream is reduced to a dribble |
| Paraphimosis | ||
| Balanitis |
Case 29.3
Lymph nodes, a common source of neck lumps, are not usually midline.
Case 29.4
All intrinsic hand muscles are supplied by the ulnar nerve, except:
The extrinsic hand muscles are supplied by median, ulnar and radial nerves:
| Action | Muscles responsible | Innervation |
|---|---|---|
| Opposition of thumb | Opponens pollicis | Median and ulnar |
| Abductor pollicis brevis | ||
| Flexor pollicis brevis | ||
| Extension of thumb | APL, EPB, EPL | Radial |
| Abduction of thumb | Abductor pollicis brevis | Median |
| Flexion of thumb | Flexor pollicis brevis | Median and ulnar |
| Adduction of thumb | Adductor pollicis, 1st palmar interosseous | Ulnar |
| Flexion of fingers at MCP | Lumbricals Palmar interossei Dorsal interossei | Ulnar (medial 2) and median (lateral 2) Ulnar Ulnar |
| Extension of fingers at MCP joints | ED, EI, EDM | Radial |
| Abduction of fingers at MCP joints | Dorsal interossei | Ulnar |
| Adduction of fingers at MCP joints | Palmar interossei | Ulnar |
| Flexion of fingers at PIP joints | FDS | Median and ulnar |
| FDP | Median | |
| Flexion of fingers at DIP joints | FDP | Median and ulnar |
| Extension of fingers at IP joints | Lumbricals | Median and ulnar |
| Palmar interossei | Ulnar | |
| Dorsal interossei | Ulnar | |
| Abducts little finger | Abductor digiti minimi | Ulnar |
| Flexes little finger | Flexor digiti minimi | Ulnar |
| Draws 5th digit forward and rotates it so it can meet the opposing thumb | Opponens digiti minimi | Ulnar |
| Flexion of hand | FCR | Median |
| FCU | Ulnar | |
| (Also FDS, FDP, PL, FPL to a lesser degree) | ||
| Extension of hand | ECU, ECRL, ECRB, (ED, EDM, EI, EPL, EPB to a lesser degree) | Radial |
It is most likely to be due to a peripheral nerve lesion, as a pathology originating from the spinal cord or nerve root would usually involve more than one peripheral nerve. For example, damage at C8 or T1 spinal cord and/or nerve root level would not only affect the ulnar nerve (formed from nerve roots C7–T1), but it would also affect the median nerve (formed from nerve roots C5–T1) and radial nerve (formed from nerve roots C5–T1). This is best explained by understanding the anatomy of the brachial plexus, illustrated in Figure 29.1.
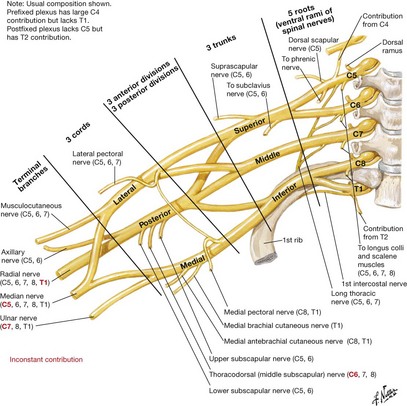
Figure 29.1
(Source: Netter illustration from www.netterimages.com. © Elsevier, Inc. All rights reserved.)
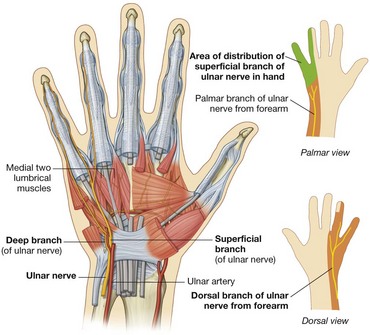
This would be on both the palmar and dorsal surface of the little finger, medial half of ring finger, and its corresponding area on the hand. Figure 29.2 depicts the sensory distribution of the ulnar nerve.




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


