An estimated 850,000 meniscal procedures are performed yearly in the United States.
Although meniscus preservation is always preferable, large irreparable tears often require partial or subtotal meniscal excision.
Many patients will become symptomatic in the meniscaldeficient compartment resulting from increased articular cartilage contact stresses and progressive cartilage deterioration.
Medial meniscus deficiency may decrease the contact area in the compartment by 50% to 75% and increase the contact stress by 134% to 200%.1,8
Lateral meniscus deficiency can decrease the contact area in the compartment by 45% to 50% and increase the contact pressure twofold.13
Meniscal allograft transplantation is an option in the carefully selected patient with symptomatic meniscal deficiency prior to the development of advanced degenerative change.
The menisci are semilunar fibrocartilaginous discs made of predominantly type I collagen. Water, which accounts for 70% of meniscal composition, is trapped within the matrix by negatively charged glycosaminoglycans (FIG 1).
Typically, only the peripheral third of the meniscus is vascularized (10% adjacent to popliteal hiatus). Blood supply is via the perimeniscal capillary plexus with contributions from the superior and inferior medial and lateral geniculate arteries.
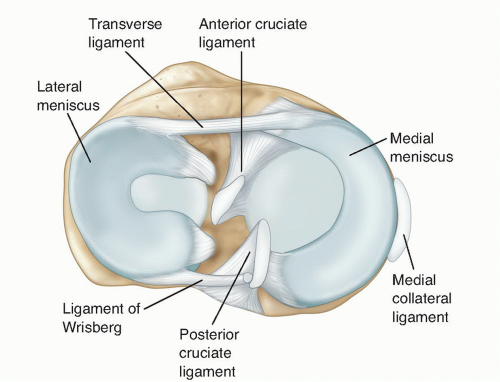
FIG 1 • Meniscal anatomy.
Medial meniscus
The medial meniscus covers a smaller percentage of medial compartment surface than the lateral meniscus.
A portion of the anterior cruciate ligament (ACL) tibial insertion footprint lies between the anterior and posterior horn attachment sites. This is typically a small percentage.
Lateral meniscus
The lateral meniscus covers a relatively larger percentage of the articular surface in its respective compartment than the medial meniscus.
The anterior horn attaches adjacent to the ACL and the posterior horn attachment is behind the intercondylar eminence.
The anterior and posterior horn attachments are closer to each other than the medial meniscus without a ligament insertion footprint interposed between the two sites. This makes the lateral meniscus more amenable to a bone bridge transplantation technique.
A discoid variant is found in 3.5% to 5% of patients.
Meniscal pathology is generally of two types:
Acute traumatic tears
These injuries typically occur in a previously relatively “healthy” meniscus in patients younger than 35 years old; however, they may also occur in older individuals.
Traumatic tears often include unstable longitudinal tears within the vascular zone, which are optimal candidates for meniscal repair.
They often occur in association with combined knee injuries (ACL, medial collateral ligament).
Degenerative tears
This is a more complex tear pattern that typically occurs in patients older than 35 years old.
Often, a relatively minor trauma or event “breaks the camel’s back” and a tear propagates through degenerative meniscal tissue.
These are typically not repaired.
Risk factors for meniscal tears include sports participation (especially jumping and cutting sports, which increases the risk of concurrent ACL injury), age, higher body mass index, occupational kneeling and squatting (associated with degenerative rather than acute traumatic meniscal lesions), level of activity, and ACL instability.
The association of meniscal tears with ACL tears is well documented. Lateral meniscal injuries occur more frequently with acute ACL disruption, whereas medial meniscal injuries occur more often in the setting of chronic ACL insufficiency.
Irreparable tear patterns or failed previous meniscal repairs often necessitate arthroscopic meniscal excision of the unstable tear component. The degree of tear propagation typically dictates the resection required.
Meniscectomy can decrease the contact area by 50% to 75% and increase joint contact stresses by 134% to 200%.1,8
Contact stresses increase and contact areas decrease as a function of the amount of meniscus that is resected. Segmental meniscectomy can decrease contact areas and increase mean and peak contact stresses as much as a total meniscectomy.8
These increases in joint contact stress often lead to premature cartilage deterioration and the development of osteoarthritis. Although patients often remain relatively asymptomatic until they have advanced degenerative changes, patients (who tend to be younger and more active) can develop pain earlier in the degenerative process.
Lateral meniscectomy is considered to have a poorer prognosis than medial meniscectomy.
The medial meniscus is the secondary stabilizer to anterior tibial translation. Medial meniscectomy (posterior horn) in the ACL-deficient knee often increases tibial translation and instability.
Potential transplant patients are typically younger, have an absent or nonfunctioning meniscus, and are symptomatic from their meniscal insufficiency.
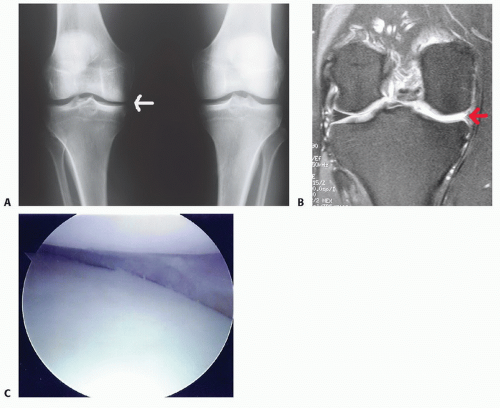
FIG 2 • A. AP weight-bearing bilateral knee views showing subtle medial compartment joint space narrowing of the right knee (arrow). B. MRI showing deficient medial meniscus. C. Arthroscopic image of right knee showing deficient medial meniscus.
A detailed history includes specific symptoms, prior injuries, and subsequent surgery. Arthroscopy pictures are helpful in determining the degree of meniscal resection and the condition of the articular cartilage.
Symptomatic postmeniscectomy patients typically present with joint line pain (sometimes subtle), swelling, and pain associated with barometric pressure changes. Symptoms are usually activity related.
The physical examination should focus on determining pain location, ligament stability, alignment, and ruling out alternative causes of pain in the differential diagnosis.
Palpating the joint line for tenderness will help localize the source of pain.
Sharp pain on the McMurray test may indicate recurrent meniscal injury or chondral lesion versus meniscal insuf-ficiency (typically more of a dull ache).
The Lachman test assesses for concomitant ACL pathology, which should also be addressed at the time of surgery.
Concerns about malalignment necessitate long-leg alignment films.
Reasonably symmetric range of motion and adequate muscle strength should be obtained prior to the transplantation.
Range of motion should not be significantly limited in a potential transplant patient.
Plain radiographs: initial imaging modality
Anteroposterior (AP) view of both knees in full extension (FIG 2A): Look for subtle joint space narrowing.
Rosenberg view: weight bearing, 45-degree flexion posteroanterior view: Look for subtle joint space narrowing.
Merchant view
Non-weight-bearing lateral views
Long-leg alignment films (if malalignment is suspected)
Magnetic resonance imaging (MRI): to assess menisci, articular cartilage, and subchondral bone (FIG 2B)
Bone scan can be considered and may reveal increased activity in the involved compartment. However, it is not typically used and its sensitivity in this setting is unknown.
Diagnostic arthroscopy is often recommended.
It will accurately define the extent of meniscectomy and the degree of arthrosis if previous arthroscopic images are unavailable or unclear or if more than 6 months to 1 year has elapsed since the last arthroscopy (FIG 2C).
Outerbridge grade III or less articular cartilage damage is acceptable (grade I or II is preferable). A focal grade IV lesion may be addressed concurrently with a cartilage resurfacing procedure. Diagnostic arthroscopy may also assist in planning the optimal method for addressing the articular cartilage lesion.
Recurrent meniscal tear
Chondral or osteochondral lesion (may be the primary cause of pain but may require chondroprotection of meniscus transplant)
Advanced bipolar degenerative chondrosis
Synovitis
Patellofemoral pain (radiating medial)
Extra-articular sources (ie, pes tendinitis)
Hip or spine pathology
Activity modification (nonimpact activities and exercises)
Appropriate pharmacologic therapy
Injection therapy (may be helpful for differentiating between intra- and extra-articular sources of pain)
Unloader braces
A potential exception to nonsurgical management may be in the setting of the chronically ACL-insufficient knee or failed ACL-reconstructed knee with medial meniscal deficiency.
A concomitant reconstruction of the ACL with a meniscal allograft transplant may improve joint stability, ACL graft survival, and eventual clinical outcome.
This is a new relative indication.
Indications are patients typically younger than 50 years of age with an absent or nonfunctioning meniscus and with pain due to meniscal insufficiency or progressive joint space narrowing, prior to the development of advanced chondrosis. Less than 2 to 3 mm of joint space narrowing on weightbearing films is ideal.9
Younger patients, younger than 30 years of age, with progressive joint space narrowing following meniscectomy presenting with less severe pain may be considered as candidates.
Additionally, patients with a failed prior ACL reconstruction or severe chronic ACL instability combined with medial meniscus deficiency may be candidates for combined ACL reconstruction and meniscus transplantation. Typically, these patients have fairly pronounced anterior laxity on their examination.
Upper limit for age is generally 50 years for highly active patients who are not good candidates for arthroplasty.
Contraindications to surgery include immunodeficiency, skeletal immaturity, inflammatory arthritis, prior deep knee infection, osteophytes or flattening of the involved condyle indicating bony architectural changes, marked obesity, diffuse Outerbridge grade IV articular changes (focal chondral defects can be addressed concurrently), knee instability, or marked malalignment (unless these issues are corrected).
Graft sizing: Although size matching of meniscal allografts to recipient knees is thought to be critical, the tolerance of size mismatch is unknown, and currently, no single measurement method is accepted. A general recommendation is to attempt to use an allograft that is within 5% of the patient’s native meniscal size. Tissue banks will often calculate the graft size using unpublished, proprietary formulas9; however, most surgeons should confirm the sizing using various measurements based on plain radiographs, computed tomography (CT), or MRI (Table 1).
The Pollard method, the current reference standard, uses the bony landmarks seen on plain radiographs and calculates the meniscal dimensions after correcting for the radiograph’s magnification and multiplying by a factor of 70% and 80% for a lateral and medial meniscus, respectfully.15
Table 1 Meniscal Allograft Sizing Methods
Sizing Method
Strengths and Weaknesses
Direct measurement
Contralateral knee may be used for sizing, although some variability exists in menisci of opposite knees.
Plain radiographs
The consistent relationship between meniscal size and landmarks in plain radiographs often is used by tissue banks for allograft sizing.
By using measurements of the length and width of the medial and lateral tibial plateaus, McDermott et al11 determined that meniscal size can be predicted with a mean error rate of 5%.
MRI
Prodromos et al16 showed that contralateral MRI better predicts meniscal size compared to plain radiographs. Although MRI is historically considered slightly more accurate at sizing allografts when compared to plain radiographs, Shaffer et al20 still found that only 35% of menisci measured with MRI were within 2 mm of the actual size needed.
CT
Carpenter et al2 reported that MRI consistently underestimated the anteroposterior and mediolateral sizes of both the medial and lateral menisci but was more accurate in estimating meniscal height. They concluded that CT and plain radiographs were more useful in allograft sizing.
3-D CT reconstruction
McConkey et al10 reported that 3-D CT has less error in measuring the tibial plateau when compared with plain radiographs. Estimations of the tibial plateau were more likely to be within 2 and 5 mm of the actual size when measured with 3-D CT than with radiographs.
MRI, magnetic resonance imaging; CT, computed tomography; 3-D, three-dimensional.
MRI, CT, and three-dimensional CT scans have been used with success as well.
Meniscal allografts are procured under strict aseptic conditions within 12 to 24 hours of cold ischemic time in accordance with standards established by the American Association of Tissue Banks for donor suitability and testing. Nonirradiated fresh frozen (most common and senior authors’ preference) or cryopreserved meniscal grafts obtained from a reputable, fully accredited tissue bank is currently recommended as these two grafts offer the highest success rates.9
Meniscal allograft survival and outcomes have not been affected by lack of donor cell viability.
The surgeon should be aware of the tissue bank’s processing procedures prior to surgery.Related posts:
 Arthroscopic Treatment of Posterior Shoulder Instability
Arthroscopic Treatment of Posterior Shoulder Instability
 Glenoid Bone Graft for Instability with Bone Loss
Glenoid Bone Graft for Instability with Bone Loss
 Snapping Hip/Lateral Hip
Snapping Hip/Lateral Hip
 Repair of Acute and Chronic Patella Tendon Tears
Repair of Acute and Chronic Patella Tendon Tears
 Anterior Cruciate Ligament Reconstruction in the Skeletally Immature Patient
Anterior Cruciate Ligament Reconstruction in the Skeletally Immature Patient
 Modified Brostrom and Brostrom-Evans Procedures
Modified Brostrom and Brostrom-Evans Procedures

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


