Fig. 24.1
(a) Phase I ROM: forward elevation. (b) Phase I ROM: ER
As stated earlier, the surgeon may delay beginning these ROM exercises until 4–6 weeks post-op for some patients with medium, large, or massive cuff tears. In these patients, the program remains the same, but the time frame for the implementation of the exercises is changed to correspond with the start date of the exercises.
Phase II
This stage typically begins 6–8 weeks after surgery for partial and small repairs and 8–12 weeks for medium, large, or massive tears. Patients are asked to continue performing the phase I ROM exercises. The supine forward elevation exercise may now be performed with a cane or stick to achieve end-range forward elevation PROM. Patients are instructed in phase II ROM exercises (Fig. 24.2) and Phase I strengthening exercises at this time (Fig. 24.3). Caution must be employed with patients who have had large or massive rotator cuff tears. Restrictions in internal rotation ROM are to be expected due to the nature of the repair. Therefore, this exercise must be performed submaximally. Pain or weakness with the strengthening exercises may necessitate shorter arcs of motion. In some cases of a complex repair or where the integrity of the repair may be in question, rotator cuff strengthening may not be initiated until 10–12 weeks post-surgery.
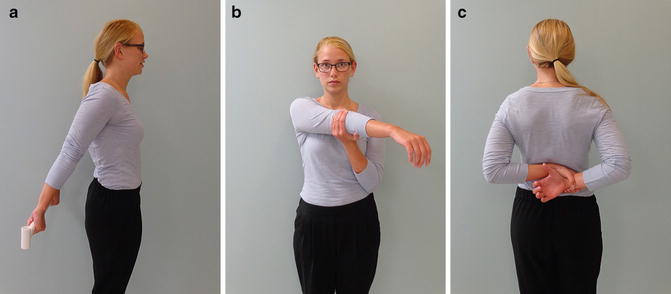
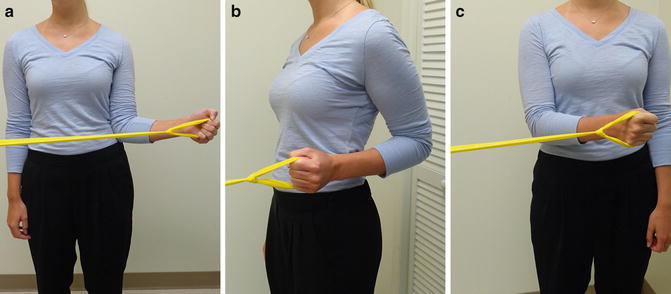
Fig. 24.2
(a) Phase II ROM: extension. (b) Phase II ROM: cross body adduction. (c) Phase II ROM: internal rotation
Fig. 24.3
(a) Phase I strengthening: external rotation. (b) Phase I strengthening: extension. (c) Phase I strengthening: internal rotation
Patients who are not progressing as expected may be referred to supervised therapy. Strengthening exercises may be delayed if the patient continues to have pain and stiffness. To help advance PROM, glenohumeral mobilizations and gentle, relatively pain-free manual stretching can be performed. To augment strengthening, manual resistance can be applied with alternating isometrics beginning with the arm supported at 45° in the plane of the scapula (POS) and neutral rotation. Scapular strengthening exercises can also begin at this time period. Exercises should be performed with the arms below shoulder height to avoid increasing pain.
Phase III
This phase begins 12–16 weeks after surgery for small/medium tears and 16–24 weeks for large/massive tears. The patient should have full PROM for FE and ER. It should be expected that internal rotation ROM will be only slightly better than at the beginning of phase II. It is important to assess active ROM at this point.
Patients who are able to raise their arm against gravity and are able to perform the phase I strengthening exercises with green resistance band will be instructed in phase II strengthening exercises (Fig. 24.4). These exercises are designed to begin training the rotator cuff and deltoid for functional demands. However, as always, pain is respected and the intensity of the exercises must be monitored.
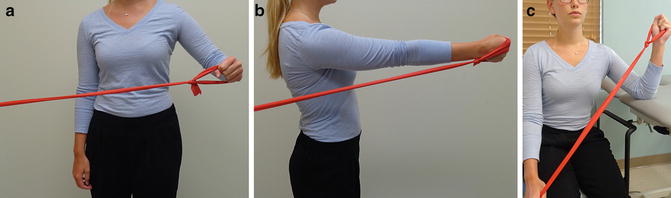
Fig. 24.4
(a) Phase II strengthening: abduction to 45. (b) Phase II strengthening: forward elevation. (c) Phase II strengthening: external rotation supported at 45
Phase IV
This phase typically begins 16–24 weeks postoperative and continues for up to 9 months postoperatively. Patients will be progressed to Phase II scapular strengthening which includes a backhand and forehand motion with elastic resistance as well as horizontal abduction with ER. Patients are encouraged to approach overhead activities with caution, and whenever possible reposition their upper extremity so that the elbow can remain below shoulder level. They are again instructed in the biomechanics of lifting in efforts to reduce the risk of rotator cuff overload.
For the athlete, sport-specific training can begin utilizing plyometrics to enhance neuromuscular control, strength, and proprioception. Recommendations and instruction for proper use of gym equipment should also be done at this time.
Rehabilitation following Arthroscopic Stabilization
Success during rehabilitation following any orthopedic surgical procedure is dependent upon the appropriate application of stress to the repaired structures. Initially minimal stress is required for beginning healing, followed by a progressive gradual increase in stress over several months to the surgical repair to protect it while the repair matures. Four principles are of critical importance for the rehabilitation professional to understand and successfully apply to be able manipulate stress and facilitate healing in capsulolabral repairs of the shoulder and promote a safe return to function: (1) a basic understanding of the surgical procedure; (2) an understanding of the anatomic structures which must be protected, how they are stressed, and the rate at which they heal; (3) the identification and skilled application of the methods used during rehabilitation to manipulate stress to the surgical repair; and (4) identifying the appropriate length of immobilization and rate of return to full ROM.
Phase I
The goals of this early phase include protecting the structures that were repaired and improving ROM in a slow controlled manner. Rapid and excessive progression of ROM may lead to a poor outcome. The evaluation is limited to passive forward elevation and passive external rotation with the arm at approximately 20° of abduction in the POS. It is also important to administer a self-report outcome tool such as the Penn Shoulder Score or ASES Shoulder Score Index at 2- to 4-week intervals in order to track progress. Patient education is important in the early phases following surgery. Patients are instructed to use their arm for waist level activities when tolerated. They are cautioned about using the arm away from the body, sleeping on the operated side, leaning on that side, and making sudden movements. When sitting, the patient is encouraged to position the arm in neutral rotation and the POS supported by a pillow.
Patients may begin their rehabilitation program at any time during the first six postoperative weeks. Surgeons may wish to hold off on beginning ROM exercises depending on the patient’s connective tissue elasticity in order to allow healing and protect the repair. We begin with pendulum exercises, hand squeezes, and elbow active ROM. Phase I passive ROM exercises are also begun at this time. These include supine forward elevation in the POS utilizing the opposite hand and external rotation supported at 45° in the POS utilizing a cane or stick. The goal for PROM FE is 135° and 45° for external rotation with the arm below 45° of abduction. Patients who rapidly regain ROM in this phase may be told to hold off performing these exercises during this time period. In addition, scapular retraction and scapular retraction with downward rotation exercises without resistance can be added at this time.
Phase II
Phase II of the rehabilitation process begins at approximately postoperative week 6 and extends to approximately week 12. The criteria for progression to phase II include appropriate healing of the surgical repair by adhering to the precautions and immobilization guidelines, and the staged ROM goals are met but not significantly exceeded. During this stage, phase II ROM exercises are added, which include extension behind the back with a stick, cross body adduction, and internal rotation up the back with the opposite hand or a towel. Rotator cuff strengthening exercises with elastic resistance are also introduced for smaller tears with solid structural repair. These are called phase I strengthening exercises, and include external rotation, internal rotation, and extension, all with the arm by the side (Fig. 24.3). Patients are asked to begin by performing one set of 10 repetitions. When they have no difficulty or discomfort with that first set, they can add a set with the goal of achieving three sets of 10 repetitions without difficulty. When they are able to achieve three sets of 10 without difficulty, they can move to the next level of elastic resistance. Manual resistance to external and internal rotation with the patient in supine and the arm supported at 45° in the POS can be initiated using alternating isometrics and short arc rotation.
Scapular muscle integration and appropriate scapulohumeral rhythm is encouraged in all strengthening exercises. Scapular retraction with elastic resistance at waist level and from overhead may be added for the middle and lower trapezius muscles. When the patient is able to achieve the third level of elastic resistance, phase II strengthening exercises can be added to the program. These include abduction with the elbow bent to 90° in the POS and staying below 60°, forward elevation to 60°, and external rotation supported at 45° in the POS (Fig. 24.4).
Phase III
Phase III of the rehabilitation program begins approximately at week 12 and extends to approximately week 24. The criteria to begin phase III include full active ROM for forward elevation, the ability to perform strengthening exercises without difficulty, and the ability to demonstrate good scapular control during the exercises and functional activities. Manual resistance can be progressed to unsupported positions, combinations of movement, and functional positions. Diagonal patterns (D1 and D2) can be incorporated into the manual resistance program. The isotonic strengthening exercises now progress to combination movements and functional patterns. Elastic resistance for “backhand” and “forehand” type motions to strengthen the scapular protractors and retractors can be added (Fig. 24.5). A useful exercise to help the throwing athlete prepare for return to throwing is the combination of horizontal abduction, scapular retraction, and external rotation against elastic resistance (Fig. 24.5). Functional internal rotation with elastic resistance mimicking the throwing motion is helpful to prepare for return to throwing (Fig. 24.6). We will also introduce one-arm rows for the latissimus dorsi and the lat pulldown machine to the front of the body.










