Chapter 17 Maxillofacial Injuries
Many primary care physicians are in the position of initial responsibility for the multicomplex injured patient. Although damage to thoracic or abdominal structures is often more easy to recognize, the ability to identify maxillofacial injuries is important for the complete evaluation of any trauma patient. Although not lethal per se, undiagnosed facial fractures may have potentially lethal complications or may produce contour deformities with or without functional disabilities. Automobile accidents are the most frequent cause of maxillofacial injuries and represent a high-velocity type of injury. Other modes of injury include motorcycle accidents, fistfights, sports, falls, bicycle accidents, and convulsive disorders. Identification of the cause is important, because one third of patients with maxillofacial injuries caused by motor vehicle accidents have associated life-threatening cranial, pulmonary, or intraabdominal injuries. About one third also have accompanying nonlethal injuries, such as extremity fractures or eye loss. On the other hand, patients with maxillofacial injuries secondary to low-velocity causes (assaults or falls) have a markedly decreased incidence of associated injury: life-threatening (4%) and nonlethal (10%).
Associated Injuries
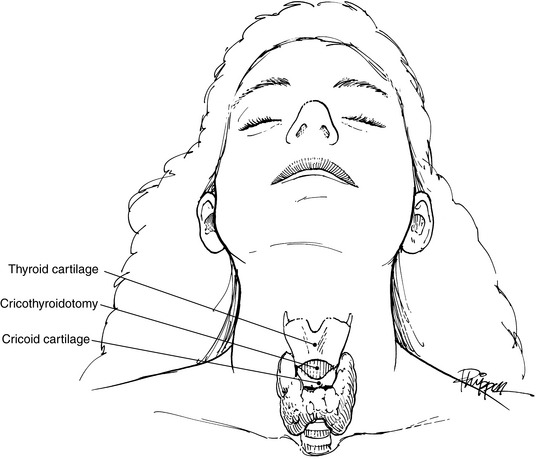
Airway obstruction with subsequent hypoxemia can easily develop in the patient with a maxillofacial fracture. Blood clots, broken teeth or dentures, and foreign bodies, such as dirt or glass, can physically obstruct the airway. The posterior displacement of the tongue secondary to the patient’s position or to a mandibular fracture may occlude the airway. Other potential causes include glossopharyngeal edema and expanding hematoma. In all situations, a patent airway must take immediate priority. Sweeping debris from the oropharynx and mouth by using one’s finger may be a lifesaving technique. Suction, if available, is helpful. Simple traction on a posteriorly displaced tongue by suture or towel clip may alleviate obstruction. If these methods fail, oral intubation must be instituted. If facial edema, facial fractures, or cervical spine fractures prevent oral or nasal intubation, a cricothyroidotomy can be performed through the membrane between the thyroid and cricoid cartilages (Fig. 17-1). This site is a bloodless field, and the procedure can easily be done in the emergency department with only a scalpel. Later, an elective lower tracheotomy can be performed under controlled circumstances in the operating room. A low tracheotomy performed in the emergency department may be very hazardous and should be avoided.
Hemorrhage from open wounds can be controlled most easily by pressure dressings consisting of layers of gauze (Kerlix) and elastic bandages. Occasionally, an active bleeder in a facial wound may need to be clamped and ligated. However, blind clamping of possible bleeding sites is condemned because of the high incidence of iatrogenic complications, such as facial nerve damage. Nasal hemorrhage may require packing. Shock occurs very seldomly from an isolated maxillofacial injury and most commonly results from a thoracic or abdominal injury.
Examination and Diagnosis
An accurate history should be obtained whenever possible from the patient and/or witnesses at the scene of the accident. The type of accident, the patient’s position in the car, the use of safety belts, the mode of impact, and the patient’s condition at the time of injury are all important considerations in the initial assessment. Because alcohol is involved in 50% of automobile accidents, a blood alcohol sample should be drawn. Ingestion of other drugs should be considered by an appropriate drug screen analysis. A review of the patient’s past history should include other illnesses, previous surgery, allergies, and all current medications.
A diagnosis of facial bone injury can be established by three methods: observation, palpation, and radiologic evaluation. Moderate to severe facial edema may mask bony irregularities and asymmetries (Fig. 17-2). After resolution of the edema, facial asymmetry is suggestive of an underlying fracture. Light manual palpation is important in making the initial diagnosis.

The Waters’ view is the single most informative roentgenogram in evaluation of the maxillofacial patient in the emergency department (Fig. 17-3). This study visualizes the floor and rims of the orbits, the walls of the sinuses, the zygomatic bones, the zygomatic arches, and the nasal septum with minimal interference of other bony structures. Opacity of a maxillary sinus suggests hemorrhage as a result of an orbital ridge and/or floor fracture. The Waters’ view requires the cooperation of the patient and a normal cervical spine, however, because the patient must be in the prone position during the examination. If the patient is comatose, uncooperative, or suspected of having a cervical fracture, a reverse Waters’ view with the patient in the supine position is a satisfactory substitute, because it gives almost the same level of detailed information. Other films worth consideration in the emergency department are the submental vertex view of the zygomatic arches and a mandible series. More sophisticated and detailed studies can be obtained later during the hospitalization or on an outpatient basis for isolated facial fractures.

Since the development of computed tomography (CT) scanning, it has become essential for the diagnosis of facial trauma. The CT scan is a more accurate diagnostic study and allows an evaluation of complicated facial fractures before the resolution of edema. Additionally, injuries to the soft tissue structures in the area of trauma can be better evaluated— for example, the optic nerve or orbital herniation of the orbit (Fig. 17-4).

The only disadvantage to the use of the CT scan is seen when artifacts caused by either dental fillings or metal appliances occur. Radiation is not considered a disadvantage; CT exposes the patient to a radiation dosage equal to the amount from linear tomography. Studies suggest that the amount of radiation from either study is less than the amount needed to cause cataracts.
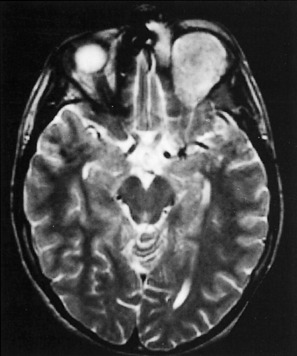
The role of magnetic resonance imaging (MRI) in the craniofacial injury patient is primarily confined to evaluation of soft tissue trauma. When injuries to the ocular structures are noted and disturbances of vision are present, MRI may help localize the site of the injury (Fig. 17-5).
Fractures of the Mandible
Although it is the thickest and heaviest of the facial bones, the mandible is the second-most commonly fractured (after nasal bones). Mandibular fractures may occur as isolated injuries or as components of complex maxillary and mandibular fractures. The most common causes of mandibular fractures are acts of violence that may range from simple falls to motor vehicle accidents. Occasionally, systemic diseases such as hyperparathyroidism and osteomalacia may predis pose to mandibular fractures. Infrequently, benign or malignant tumors, cysts, or osteomyelitis may precipitate such fractures.
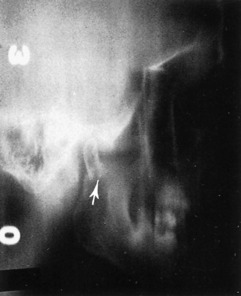
Although the clinical examination most frequently establishes the diagnosis of mandibular fractures, roentgenographic studies more clearly define the direction of the fracture line, the relationship of the teeth to the fracture, and the degree of displacement. Posteroanterior and oblique lateral views of the mandible demonstrate fractures of the body and the angle without difficulty. If available, a Panorex view of the mandible is an excellent and necessary study that shows fractures at any site. Fractures of the temporomandibular joint and condylar area are sometimes difficult to demonstrate on routine mandibular roentgenograms, however, and may require tomograms for the final diagnosis (Fig. 17-6).
The principles of treatment for mandibular fracture include early anatomic reduction of the fracture, immobilization, and control of infection. An isolated mandibular fracture should be reduced at the time of injury. However, if other life-threatening injuries are present, treatment of the mandibular injury may be postponed for 7 to 10 days. All mandibular fractures are considered compound if the slightest displacement is present, and consequently, preoperative and postoperative antibiotics are recommended. Immobilization requires at least the application of arch bars and intermaxillary fixation (IMF) with rubber bands or wires for a minimum of 5 weeks. Rigid fixation with plates or screws is an option. Because IMF is not usually required after rigid stabilization, patients are able to begin a soft diet almost immediately after open reduction. Consequently, the weight loss and compromised oral hygiene present in patients with IMF are markedly reduced. The use of compression plates has also made the treatment of edentulous patients with mandible fractures much simpler.
Fractures of the Maxilla
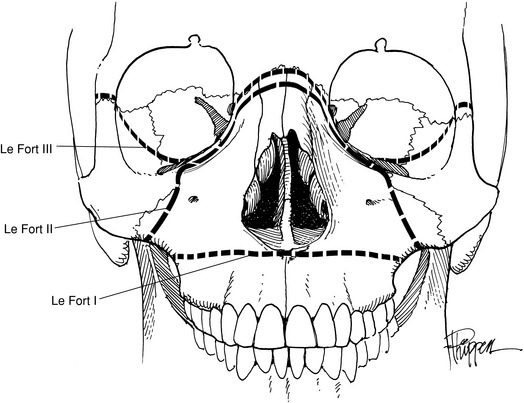
Maxillary fractures can be divided into two groups: vertical and horizontal. Vertical fractures split the palate on either side of the septum. However, the three classic fractures of the maxilla are those horizontal defects described by Le Fort (Fig. 17-7). The Le Fort I (transverse) fracture is a horizontal fracture immediately above the level of the teeth. The Le Fort II fracture has the configuration of a pyramid, with the apex being across the nasal bridge. It extends through the nasal bones, the frontal processes of the maxilla, the lacrimal bones, the inferior rim and floor of both orbits, and the maxillozygomatic suture line. From this last point, the fracture continues posteriorly through the lateral wall of the maxilla and the pterygoid plates into the pterygoid maxillary fossa. The Le Fort III fracture separates the craniofacial complex and extends through the zygomaticofrontal, maxillofrontal, and nasofrontal suture lines, the floors of the orbit, and the ethmoid and sphenoid bones (Fig. 17-8).

Roentgenographically, the Waters’ view is the most reliable in demonstrating maxillary fractures in the emergency department. For vertical or alveolar fractures, occlusal views are more suitable. CT scans of the facial bones more accurately detail the full extent of the fractures. The study is usually done in the coronal view and shows the amount of the comminution, the degree of rotation, and the extent of displacement of the fracture segments (Figs. 17-9 and 17-10). Additionally, injury to the optic nerve or fat herniation may be visible.











