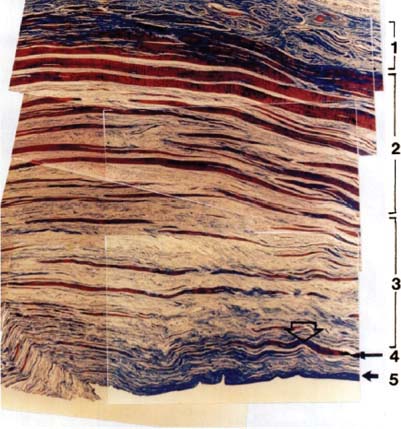
2 Massive Irreparable Rotator Cuff Tears The etiology of massive rotator cuff tears is multifactorial and continues to be a researched topic. To understand this topic requires a basic knowledge of rotator cuff (RC) histopathology. A clear understanding of the normal anatomy of the RC will aid in the treatment of the diseased cuff. Clark and Harryman1 have described the RC in detail. From their work, we know that as the tendons of the posterior cuff approach their site of insertion, they are confluent and not easily separated. Their studies have shown that the RC is made up of multiple, confluent tissue layers functioning in concert. Histological sections through the supraspinatus and infraspinatus reveal five distinct layers (Fig. 2–1). The most superficial layer contains large arterioles and comprises fibers from the coracohumeral ligament. A sheet of fibrous tissue from the coracohumeral ligament’s origin extends posterolaterally to form a sheet over the supraspinatus and infraspinatus. This layer is 1 mm in thickness and the tissue fibers are oriented obliquely to the long axis of the muscle bellies. Layer 2 is 3- to 5-mm thick and represents the direct tendinous insertion into the tuberosities. Large bundles of densely packed parallel tendon fibers compose this layer. Layer 3 is ~3-mm thick and comprises smaller bundles of collagen with a less uniform organization. Fibers within this layer travel at 45-degree angles to one another to form an interdigitating meshwork that contributes to the fusion of the cuff tendon insertion. Layer 4 comprises loose connective tissue and thick collagen bands that merge with the coracohumeral ligament at the most anterior border of the supraspinatus. Layer 5 (2-mm thick) represents the shoulder capsule. With respect to the blood supply, the arterioles are larger and the vessels more prevalent on the bursal surface of the cuff and branch between layers 2 and 3.1 The articular side of the RC is relatively hypovascular when compared with the rich blood flow on the bursal side of the cuff.2 Histologically, tendon regions subject almost exclusively to tension differ from those exposed to high levels of compression as well as tension.3 Tendons not subject to compression consist primarily of spindle-shaped fibroblasts surrounded by densely packed, longitudinally oriented collagen fibers principally made up of type I collagen. In contrast, tendons exposed to compression have a fibrocartilaginous structure and a composition characterized by rounded cells surrounded by a matrix containing type I and type II collagen, chondroitan-4-sulfate, and chondroitan-6-sulfate.4 Figure 2–1 Vertical, transverse section through the supraspinatus tendon and capsule near the tendon insertion. Layer 1 is composed of fibers of the coracohumeral ligament obliquely oriented with respect to the axis of each muscle. Large arterioles are present. Layer 2 is composed of closely packed parallel tendon fibers grouped in large bundles. Layer 3 has smaller fascicles and these fascicles lack a uniform orientation. Blood vessels are also present in this layer, but are smaller than those in layers 1 and 2. Layer 4 is composed of loose connective tissue in which there are thick bands of collagen fibers. The only blood vessels in this layer are capillaries, found adjacent to the extraarticular surface of the capsule of the shoulder. Layer 5 is a thin, continuous sheet of interwoven collagen fibrils, which usually insert on the humerus as Sharpey’s fibers within the bone. Degeneration of the RC is a common source of shoulder dysfunction. It has been demonstrated that the presence of RC pathology was highly predictive of impaired physical health and quality of life.5–7 In fact, the size of this impact is comparable to the effects of conditions such as diabetes mellitus, myocardial infarction, congestive heart failure, hypertension, and clinical depression.6 Patients with massive RC tears generally present with complaints of pain and weakness. Large tears increase the likelihood of functional loss. Recent studies have shown that weakness of >50%, relative to the contralateral side in shoulder abduction at 10% of abduction, was indicative of a large or massive RC tear.7 MacDermid et al8 have demonstrated that patients with RC pathology were weaker than the control group of subjects who displayed no shoulder problems. Patients often complain of pain with activity, as well as night pain. Physical pain is the result of the inflammatory nature of the subacromial bursa in RC disease. The expression of inflammatory mediators known to be involved in the catabolic degenerative processes in the subacromial bursa was studied and quantified in bursal specimens in patients with RC disease. The data clearly show increased inflammation in the subacromial bursa in patients with RC disease when compared with control patients. All of the cytokines, proteases, and cyclooxygenase enzymes that were tested showed significantly increased expression in the RC group than in the control group.9 These enzymes may play an important role in the ultimate failure of the RC. Chronic massive tears have associated osteopenic bone, poor-quality tendons, and inelastic muscles due to fatty infiltration and fibrosis.10 In fact, the weakest link in the aged may be the osteoporotic bone. Bone density is higher below the articular than in the greater tuberosity, and tendon tears are associated with a reduction of cancellous bone density of greater than 50%.11 In addition to bone quality, age also plays a role when analyzing the results of tendon repair. In patients with isolated supraspinatus tears who underwent arthroscopic repair, age was clearly one of the most important variables for tendon healing. In a study by Boileau et al,12 only 10 of 23 patients (43%) over the age of 65 had completely healed tendons. Established full-thickness tears of the RC do not heal.13 Most tendon-to-bone healing models document that contact between the bone and the residual stump of the torn tendon is necessary for healing to occur.14
Anatomy of the Rotator Cuff
Prevalence
Natural History
Related posts:
 The Spectrum of Disease in the Rotator Cuff–Deficient Shoulder
The Spectrum of Disease in the Rotator Cuff–Deficient Shoulder
 Muscle Transfers for the Treatment of the Irreparable Rotator Cuff Tear
Muscle Transfers for the Treatment of the Irreparable Rotator Cuff Tear
 Classification of Rotator Cuff– Tear Arthropathy
Classification of Rotator Cuff– Tear Arthropathy
 Rationale and Biomechanics of the Reversed Shoulder Prosthesis: The French Experience
Rationale and Biomechanics of the Reversed Shoulder Prosthesis: The French Experience
 Arthroscopic Management of Massive Rotator Cuff Tears
Arthroscopic Management of Massive Rotator Cuff Tears
 Treating the Rotator Cuff–Deficient Shoulder: The Florida Orthopaedic Institute Experience
Treating the Rotator Cuff–Deficient Shoulder: The Florida Orthopaedic Institute Experience
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


