Managing Poor Tissue and Bone Quality in Arthroscopic Rotator Cuff Repair
The majority of rotator cuff tears occur in individuals over the age of 65. As our population increases in size and advances in age, so too will the number of rotator cuff tears. A growing number of people are remaining active as they age, frequently continuing to place substantial physical demands on their shoulders into their seventh and eighth decades of life. At the same time, the rotator cuff undergoes intrinsic degeneration and the prevalence of osteoporosis increases. Consequently, a significant and growing number of rotator cuff repairs are performed in individuals with poor soft tissue or bone quality. Moreover, while the majority of rotator cuff tears occur at the tendon–bone insertion, fixation quality can be challenged by a tear that occurs more medially, leaving only a small amount of tendon for fixation by suture.
Biologic factors (e.g., poor healing potential) have often been implicated in retearing following rotator cuff repair and have led to attempts to augment healing by means of biologic modalities such as platelet-rich plasma and rotator cuff patches. While retearing certainly increases with advancing age, we believe that biologic explanations (1) for failure of rotator cuff repair have too often been used as excuses for an inadequate repair. We have found that with adherence to basic biomechanical principles, and the occasional use of some advanced tricks, adequate fixation can be achieved in the majority of cases, even in the setting of poor soft tissue quality and osteoporotic bone.
MANAGING POOR SOFT TISSUE QUALITY
Multiple Fixation Points
When soft tissue quality is poor, we prefer to make multiple sutures passes through the rotator cuff and tie as many knots as possible. Increasing the number of points of fixation is one of the simplest ways to improve construct strength. With multiple fixation points, the load per fixation point is decreased, and thus the load the soft tissue must resist to prevent cutout is similarly decreased. Because the number of suture anchors that can be placed in bone is limited by the size of the bone bed, the best way to increase the number of fixation points in the repair construct is to increase the number of sutures by use of double-loaded suture anchors.
For example, based on average cross-sectional areas and muscle contraction, a 4-cm-long rotator cuff tear involving the supraspinatus and infraspinatus will experience a force of 302 N across the rotator cuff (2,3). Suppose that the rotator cuff tear is repaired with three suture anchors, 1 cm apart. If each anchor has one suture, then there are a total of five fixation points (three by suture, two by the tendon-to-bone insertions) that equally share the load of 302 N (Fig. 9.1A). In this case, each suture–rotator cuff interface must resist a load of 60.4 N. If each anchor is double loaded with two sutures, however, eight fixation points exist (six by suture, two by tendon-to-bone insertions) and each suture–rotator cuff interface must now only resist a 37.7-N load (Fig. 9.1B)
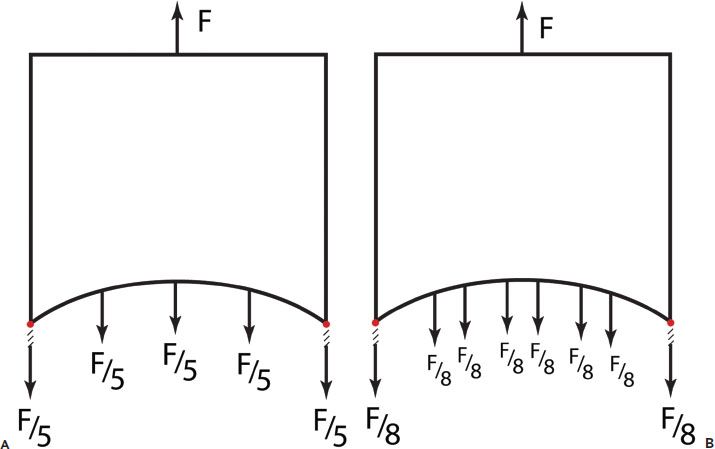
Figure 9.1 Model of three anchor fixation. A: With one suture per anchor, there are five fixation points (three by suture, two by tendon-to-bone insertions). B: With two sutures per anchor, there are eight fixation points for a three-anchor construct. F, force of rotator cuff.
It is important to remember that in order to maximize the potential of multiple sutures, the sutures should be passed separately through the rotator cuff and as many knots as possible should be tied. While current suture-bridging double-row repairs may be performed with a knotless technique, a knot increases the resistance to tissue cutout. Therefore, when performing a double-row repair in the setting of impaired tissue quality, it is advantageous to tie knots medially before securing these suture limbs laterally.
Diamondback Repair
The diamondback repair was developed by the senior author (SSB) as an enhanced suture-bridging repair construct that maximizes the concept of multiple fixation points (see Chapter 4, “Complete Rotator Cuff Repair”). This repair configuration provides twice as many linked diagonal compressive sutures with three times the number of intersection points as the standard transosseous equivalent technique (Fig. 9.2). In addition, it provides a compressive bridging mattress suture between the two medial anchors as a means to seal off the footprint from synovial fluid originating in the joint. The theoretical advantages have been borne out in biomechanical testing in which the diamondback repair construct was compared to single- and double-row repairs and demonstrated the highest initial footprint contact area and the lowest decrease in footprint area over time (4). Because footprint restoration is important for healing, this technique is useful for large and massive rotator cuff tears with impaired soft tissue quality.
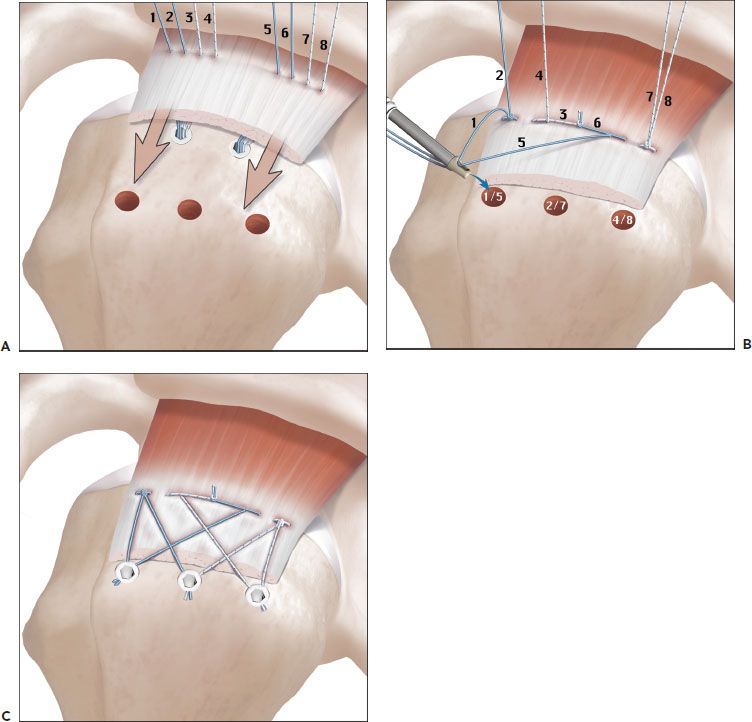
Figure 9.2 Schematic of the diamondback repair. A: Two medial screw-in anchors are placed adjacent to the articular margin of the rotator cuff footprint. All sutures are separately passed through the rotator cuff medially. B: A mattress stitch is tied between the limb of a suture from the anterior anchor and the limb of a suture from the posterior anchor. The free ends of these knotted sutures are then tensioned, utilizing the eyelets of the two anchors as pulleys to pull the knot down onto the cuff. The remaining sutures are tied as mattress stitches, but the suture tails are not cut. The remaining sutures tails are crisscrossed over the footprint by matching up suture limbs and passing each of these suture pairs through the closed eyelet of three separate knotless screw-in anchors. C: Final repair after lateral fixation demonstrates the diamondback pattern of repair.
Stitch Configuration
In order to minimize failure of suture cutting through the tendon, various “grasping-type” suture techniques have been proposed. Gerber et al. (5) reported that a modified Mason-Allen stitch was the strongest of nine different stitch patterns. Unfortunately, the inability to easily perform an arthroscopic Mason-Allen stitch has been used by some authors as justification for open repair. However, weaving suture patterns such as the modified Mason-Allen are prone to early failure by loss of loop security (6). During cyclic loading, the suture weave within the tendon tightens upon itself and the suture loop becomes larger (Fig. 9.3). The result is a loss of loop security, thus a loss of tendon–bone contact. The most efficient way to minimize cinching is to use a single loop of suture—a simple stitch.
A “rip-stop” suture is an effective method of avoiding cinching, while improving resistance to suture cut out. An anterior-to-posterior mattress stitch can be placed in the rotator cuff and tied on itself. Subsequently, simple sutures from an anchor are passed medial to the rip-stop suture that distributes the medial-to-lateral tensile forces and effectively decreases the chance of suture cut out (Fig. 9.4). Such a rip-stop suture may be placed as an isolated suture or with the use of a double- or triple-loaded anchor. In the case of an anchor, the first set of anchor sutures are used to create a mattress stitch and the remaining sutures are passed medial to lateral in a simple pattern. Ma et al. (7) demonstrated that a rip-stop suture with a double-loaded anchor had a load to failure equivalent to a modified Mason-Allen stitch. In a follow-up study, it was reported that a triple-loaded anchor with a horizontal rip-stop stitch and two simple stitches demonstrated even less elongation with cyclic loading (i.e., maintained loop security) and a higher ultimate load to failure compared to the rip-stop configuration with a double-loaded anchor (8). Notably, however, the highest load to failure was observed with a classic double-row repair.
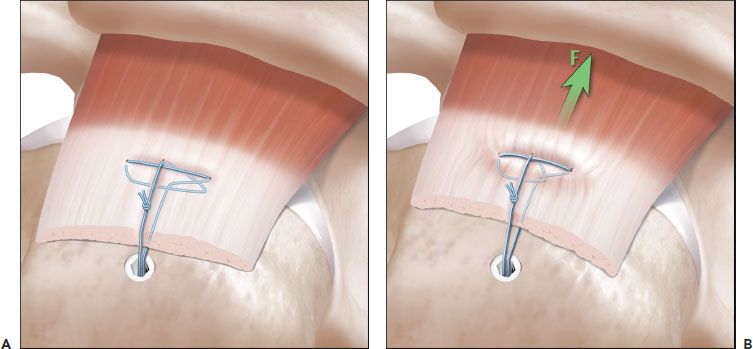
Figure 9.3 Schematic of a modified Mason-Allen stitch. Although this stitch pattern has a high load to failure, it has poor loop security under load. A: A modified Mason-Allen stitch based off an anchor has been woven through the rotator cuff. B: Under a medial tensile load (F), the complex weave cinches upon itself, resulting in loss of loop security and thus medial displacement of the rotator cuff.
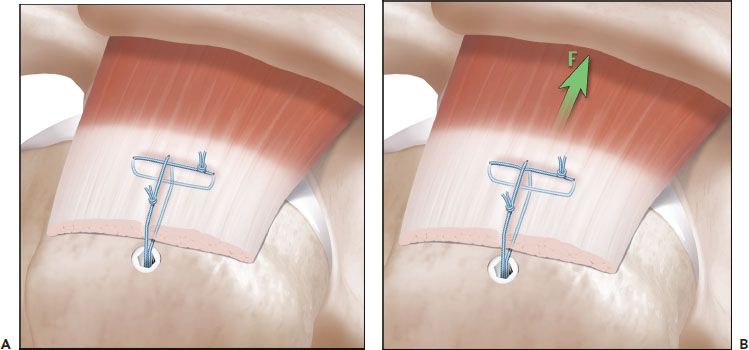
Figure 9.4 Schematic of a rip-stop stitch. This stitch pattern increases pullout and maximizes loop security by using only simple stitch loops. A: A simple stitch is placed from anterior to posterior through the rotator cuff perpendicular to the rotator cuff fibers. Then, a simple stitch is passed medial to the rip-stop stitch. This technique can be performed as illustrated or with both sutures based off of the anchor. B: Under a tensile load (F), the rip-stop stitch resists cutout of the simple stitch.
Load-Sharing Rip-stop Double-row Repair
We have developed a rotator cuff repair technique that combines the advantages of a wide rip-stop suture tape and a double-row repair (Figs. 9.5 and 9.6). This technique is particularly useful for cases involving medial tears in which there is limited medial tendon that precludes a standard double-row repair. One or two FiberTape (Arthrex, Inc., Naples, FL) rip-stop sutures are secured to two BioComposite SwiveLock anchors (Arthrex, Inc., Naples, FL) laterally in a modified SpeedFix repair (see Chapter 4, “Complete Rotator Cuff Tears”). The FiberTape rip-stop provides resistance to tissue cut out for simple sutures that are passed from a medial row of two BioComposite Corkscrew FT anchors (Arthrex, Inc., Naples, FL). The FiberTape is also a load-sharing construct that reduces the load that has to be resisted by the simple sutures.
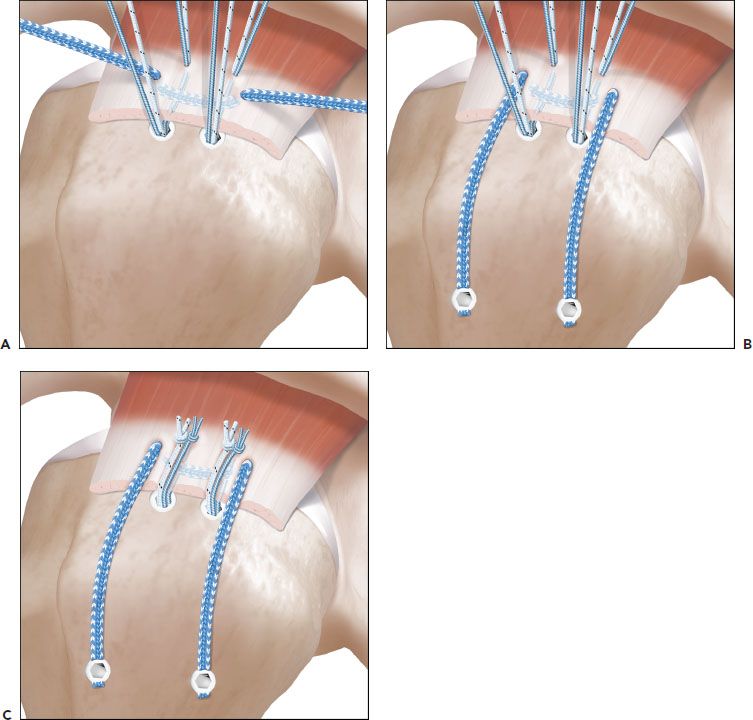
Figure 9.5 Schematic illustration of an anchor-based rip-stop rotator cuff repair for a rotator cuff tear with lateral tendon loss. A: A FiberTape (Arthrex, Inc., Naples, FL) suture has been placed as an inverted mattress stitch in the rotator cuff. Two medial anchors (BioComposite Corkscrew FT; Arthrex, Inc., Naples, FL) have also been placed and sutures from these anchors are passed medial to the rip-stop stitch. B: Prior to tying sutures from the medial Corkscrew anchors, the rip-stop stitch is secured to bone with two lateral BioComposite SwiveLock C anchors (Arthrex, Inc., Naples, FL). C: Tying the suture limbs from the Corkscrew anchors completes the repair
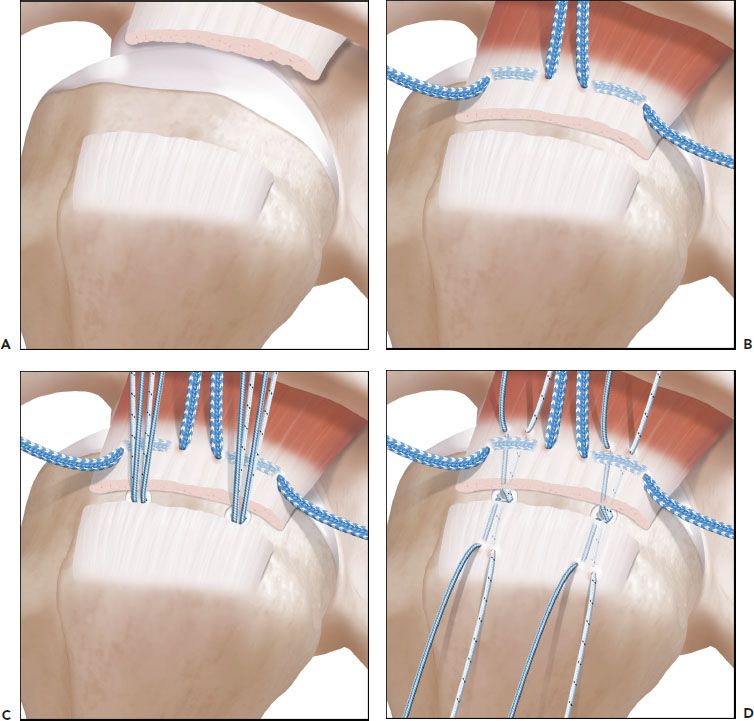
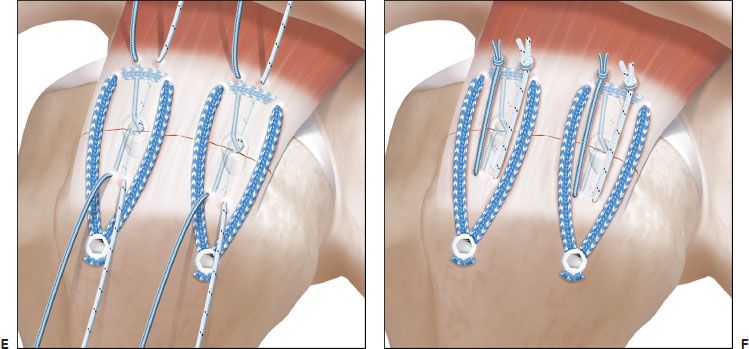
Figure 9.6 Schematic illustration of a dual rip-stop rotator cuff repair. A: In this medial rotator cuff tear with a lateral tendon stump, there is limited space to achieve fixation in the medial tendon. B: Two FiberTape (Arthrex, Inc., Naples, FL) rip-stop sutures are placed 3 mm lateral to the musculotendinous junction as inverted mattress stitches. C: Two BioComposite Corkscrew FT anchors (Arthrex, Inc., Naples, FL) are placed in the greater tuberosity bone bed. D: Suture limbs from the Corkscrew anchors are passed medial to the rip-stop stitches. In addition, the opposite suture limbs are passed through the lateral tendon stump.E: The FiberTape rip-stop sutures are secured laterally with BioComposite SwiveLock C anchors (Arthrex, Inc., Naples, FL). These rip-stop sutures are load sharing and are secured before the Corkscrew anchor sutures are tied. During this step, it is important to retrieve the rip-stop sutures so that they surround the lateral sutures limbs from the Corkscrew anchors. F: The repair is completed by tying the sutures limbs from the Corkscrew anchors.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


