Pelvic fractures in pregnant women are usually high-energy injuries associated with risk of mortality to both mother and fetus. The mother’s life always takes priority in the acute setting as it offers the best chance of survival to both the mother and the fetus. Indications for operative intervention of acute pubic symphysis rupture depend on presence of an open disruption, amount of displacement, and degree of disability. Chronic symphyseal instability related to pregnancy is a challenging problem and the first line of treatment is nonoperative care. A previous pelvic fracture is not a contraindication by itself to vaginal delivery.
Key points
- •
Pelvic trauma in pregnant women represents a life-threatening condition to both the mother and child. In the acute setting, the mother’s life takes precedence over that of the unborn child.
- •
Acute pubic symphysis rupture caused by pregnancy is rare and can usually be managed nonoperatively. However, with diastasis of greater than 4 cm, open pubic symphysis rupture, and continued pelvic malreduction in a pelvic binder, operative intervention should be considered.
- •
Chronic pelvic instability related to parturition is a common syndrome and can almost always be managed nonoperatively.
- •
In most cases, history of pelvic ring injury or pubic symphysis rupture is not a contraindication to vaginal delivery. However, women with a history of pelvic trauma do have a higher incidence of cesarean section as a result of multiple factors.
Pelvic ring trauma in the pregnant woman
Epidemiology of Trauma in Pregnancy
After primary obstetric causes, trauma is the leading cause of maternal death during pregnancy. Trauma occurs in approximately 7% of all pregnancies and is most often in conjunction with motor vehicle accidents (MVAs). Similar to the trauma-related mortality in nonpregnant women, the maternal mortality from trauma is approximately 10%, with the highest risk of maternal death occurring in the third trimester. Fetal death rates are significantly higher and have been reported to be as high as 50% to 65% in cases of severe trauma.
Fetal Morbidity and Mortality
Maternal death from trauma is associated both with fetal death and a high injury severity score. If the fetus survives the initial traumatic event, it is still at a higher risk of low birth weight, premature delivery, and permanent neurocognitive dysfunction than a pregnancy not affected by a traumatic event. Multiple case reports and series have identified associations between maternal trauma during pregnancy and cerebral palsy or developmental delay in the child. This brain injury is believed to be caused by a hypoxic insult to the developing fetal brain either from maternal hypotension or placental embolus at the time of the traumatic event.
The fetus is at greater risk of death caused by trauma than the mother. Fetal demise can be caused by direct trauma, preterm labor, maternal-fetal hemorrhage, placental abruption, or uterine rupture. Before 12 weeks of gestation, the fetus is contained entirely within the bony pelvis and is protected from direct trauma. However, after 12 weeks’ gestation, direct injury to the fetus can occur through the same mechanism as the pelvic fracture. Placental abruption is the most common complication of blunt trauma in pregnancy and is responsible for fetal death in 40% to 60% of trauma-related deaths versus 1% to 5% in nontraumatic causes of fetal death. It is theorized that the force of the traumatic event causes the elastic uterine lining to separate from the inelastic placenta, interrupting the gas exchange that occurs across the placental interface. If a complete placental abruption occurs, the fetus, if viable, must be delivered rapidly in order not to deprive the fetus of oxygenated blood. Even minor trauma can increase the risk of preterm labor, placental abruption, and fetal demise, especially if the abdomen or pelvis is involved.
Prevention Strategies
Because most severe trauma in pregnant women is caused by MVAs, the best evidence-based strategy to prevent related maternal and fetal morbidity and mortality is the use of safety belts. Approximately one-half of all fetal fatalities caused by MVAs are estimated to be preventable if seat belts are worn properly. The use of seat belts has been shown to reduce the rate of preterm labor and fetal demise in pregnant women involved in MVAs. Safety belts should have both a shoulder harness and lap belt. The lap belt should sit across the pelvic brim, not the gravid uterus, and the shoulder harness should rest between the breasts.
Epidemiology of Pelvic and Acetabular Fractures in Pregnancy
Few evidence-based studies have examined the outcomes of pregnant women who sustain pelvic fractures, because such cases are rare; however, 1 large population-based study found that pregnant women who sustain pelvic fractures were at high risk for placental abruption and fetal demise. A systematic review of the literature that reported on 101 total cases of pelvic or acetabular fractures in pregnant women found that although no single institution had significant experience with this combined patient-injury demographic, maternal and fetal death were more likely to occur with MVAs and pedestrians struck by a motor vehicle than with a fall. Mortality was not affected by fracture classification (simple or complex), type (pelvic or acetabular), pregnancy trimester, or study era. In this review, the fetal mortality was 35% and the maternal mortality was 9%, which is similar to mortality from high-energy trauma in general. In a 24-year study from a major European trauma center of 4196 patients with blunt polytrauma, only 7 of the patients who sustained a pelvic fracture were pregnant (0.17% incidence in the overall population of patients with polytrauma). The mean injury severity score of these 7 women was 29.9. Five of 7 mothers survived their injuries; however, only 3 of 7 fetuses survived, and 4 were found to be deceased at the scene of the accident. In 2 of the 3 mothers in whom the fetus survived, treatment was modified based on the viability of the fetus. In all 3 cases in which the fetus survived, the mother went on to uneventful delivery of the child without any long-term effects related to the mother’s injury. Almog and colleagues found that over a 15-year period, only 15 of 1345 patients who were treated at a trauma center for a pelvic or acetabular fracture were pregnant (1.1%). One woman died of her injuries and there were 4 cases of fetal death. Four of the 15 women underwent operative fixation of their fractures, and the rest were treated nonoperatively.
Acetabular fractures are considered part of the spectrum of injuries to the pelvic ring. Most studies that have reported on acetabular fractures in pregnant women are case reports; however, Porter and colleagues reported a case series of 8 pregnant women with acetabular fractures (of a total of 518 patients) who presented to a level I trauma center over a 6-year period. Gestational age in this group ranged from 5 to 26 weeks at the time of injury. All of the patients went on to deliver at at least 36 weeks with normal Apgar scores at delivery. Long-term follow-up on the children was not reported.
Evaluation and Treatment
Initial assessment
The most unique aspect of pregnancy-related trauma is that the trauma team must simultaneously address 2 patients: the mother and the fetus. Therefore, the treatment team should include not only the standard trauma team members but also a maternal-fetal medicine specialist. The priority in a pregnant trauma patient is timely treatment and resuscitation of the mother, because this leads to better outcomes for the fetus. Standard protocol of advanced trauma life support should be adhered to by addressing airway, breathing, circulation, disability, and exposure. All female trauma patients of childbearing age should have a rapid urine pregnancy test, because sometimes neither the patient nor the trauma team may be aware of an early pregnancy. Pelvic fractures caused by high-energy mechanisms are an indicator of severe polytrauma, and there is a high incidence of associated injuries, including head, thoracic, abdominal, and spinal injuries, some of which are immediately more life-threatening than the pelvic fracture itself.
Sources of blood loss, if not obvious on physical examination, should be discovered via chest radiograph, pelvic radiograph, and focused assessment with sonography in trauma (FAST) survey. A Foley catheter should be placed to monitor adequacy of resuscitation. The presence of blood at the vaginal introitus in a pregnant trauma patient should prompt the trauma and obstetric team to rule out placenta previa, placental abruption, or labor. Nonobstetric causes include urethral or bladder injury; if a nonobstetric cause is suspected, the patient should be evaluated by a urologist before Foley catheter placement. Blood at the vagina or rectum in the presence of a high-energy pelvic fracture may also indicate an open pelvic fracture, a diagnosis that carries a mortality of near 50% and requires operative debridement and stabilization once the patient is hemodynamically stable.
Fetal considerations in the acute setting
In any pregnant women beyond the threshold of viability, continuous fetal heart rate monitoring and a maternal tocometer to monitor for uterine contractions should be used in the acute setting. Depending on the center, fetuses are typically considered viable at 24 weeks’ gestational age; however, fetuses born at less than 30 weeks are at a significantly increased risk of cerebral palsy. In obtunded or intubated patients for whom no history is available, the location of the uterine fundus allows for a close estimate of gestational age, and in early pregnancies, the standard FAST scan may be diagnostic. On secondary survey, a pelvic examination should be performed by an obstetrician, who should look for bleeding, signs of labor, and cervical length or dilation. In the setting of a pelvic fracture, such an examination may need to be performed under sedation or general anesthesia because of pain or instability. In addition, a Kleihauer-Betke (KB) blood test, which detects fetal hemoglobin in maternal circulation, can aid in detecting occult maternal-fetal hemorrhage. It is unnecessary in obvious cases of severe trauma and maternal-fetal hemorrhage, but a positive KB test should prompt the treatment team to administer Rh immunoglobulin in all Rh-negative women.
Emergent reduction of the pelvis in the pregnant patient
If an open-book pelvic fracture (anteroposterior compression type) is diagnosed on examination or radiograph, and the patient is hemodynamically unstable, a pelvic sheet or binder should be placed to tamponade presumed bleeding from disrupted pelvic vessels. The pelvis can be close reduced by internally rotating the legs and compressing on the iliac wings when applying the sheet or binder. Internally rotating the legs and holding them together by taping the knees with cushioning between them is an assistive maneuver to hold the reduction. Military antishock trousers (MAST), although effective in keeping the pelvis reduced and creating a tamponade, are no longer recommended for treatment, because they limit access to the abdomen and cannot be used for any significant period out of concern for MAST-induced lower extremity compartment syndrome.
There are several unique aspects to closed reduction of the pregnant patient’s pelvis. The gravid uterus acts as a compressive device on the inferior vena cava (IVC) when the pregnant patient is supine, which inhibits venous return and decreases cardiac output. Close reducing an open-book pelvic fracture with a sheet or a binder may worsen this problem by increasing the compression of the gravid uterus on the IVC, further decreasing venous return to the heart and cardiac output. Certain measures may help to mitigate this problem once the pelvic binder or sheet is placed. If the patient is too unstable to be placed into the full left lateral decubitus position or if there is a concurrent spinal injury preventing safe left lateral decubitus positioning, a roll or wedge may be placed under the right side of the backboard in spinal immobilized patients, or the bed rotated with the right side up. This left lateral tilt position mechanically allows the uterus to fall to the left, relieving some pressure on the compressed IVC and improving venous return to the heart and improving cardiac output by as much as 30%. There is little clinical evidence to support what degree of tilt to use ; however, the general recommendation is that 15° of left lateral tilt is acceptable. Another maneuver that may help take pressure off the IVC is for an experienced obstetrician to manually shift the gravid uterus to the left of the abdomen.
Resuscitation measures specific to a pregnant woman
Many physiologic changes during pregnancy occur and must be considered during resuscitation ( Box 1 , Table 1 ). After 20 weeks of gestation, the pregnant woman’s plasma volume is significantly increased and up to 1500 mL of blood loss can occur before hemodynamic instability becomes apparent. About 50% more fluid than usual may be required before improvement in hemodynamic status is observed. The treatment team should be aware of certain normal laboratory values in pregnant women; for instance, the normal arterial P co 2 (partial pressure of carbon dioxide) level is less than a nonpregnant patient, and if a pregnant patient’s value is in the normal nonpregnant range, hypoxia is present. If the mother’s blood type is not known, all blood products administered acutely should be Rh-negative to prevent a fetal transfusion reaction and Rh immunoglobulin should be administered. Moreover, a secondary coagulopathy or acute hypoxic event can occur as a result of amniotic fluid embolus.
First Trimester
Major organogenesis (radiosensitive)
Central nervous system development (most sensitive period)
Increased risk of teratogenesis
Increased white blood cell count may be normal
Increased erythrocyte sedimentation rate may be normal
Hypercoagulable state
Increased risk of spontaneous abortion related to general anesthesia
Second Trimester
Fetal central nervous system relatively radioresistant
Hypotension possible with supine positioning caused by aortocaval compression (as a result of increased uterus size)
Increased white blood cell count may be normal
Increased erythrocyte sedimentation rate may be physiologically normal
Hypercoagulable state
Increased risk of spontaneous abortion related to general anesthesia
Increased risk of seat belt–related injury to the fetus
Third Trimester
Maternal plasma expands by 40% to 50% (dilutional anemia)
Pregnancy-related osteoporosis possible
Increased risk of seat belt–related injury to the fetus
Increased white blood cell count may be physiologically normal
Increased erythrocyte sedimentation rate may be physiologically normal
| Parameter | Change | Implication |
|---|---|---|
| Maternal blood volume | Increased | Attenuated initial response to hemorrhage |
| Cardiac output | Increased | Increased metabolic demands |
| Uterine size | Enlarged | Potential for supine hypotension from aortocaval compression |
| Functional lung residual volume | Decreased | Hypoxemia from atelectasis |
| Gastrointestinal motility | Decreased | Greater risk for aspiration |
| Minute ventilation | Increased | Compensated respiratory alkalosis |
Continued hemodynamic instability in setting of an unstable pelvic fracture
If closed reduction of the pelvis and fluid resuscitation measures have failed to restore hemodynamic stability, there are 2 options to consider. Most often pelvic fractures result in venous plexus bleeding, which cannot be repaired surgically or embolized with angiography. In these cases, an open laparotomy with retroperitoneal packing and rapid external fixation of the pelvis can be performed to tamponade bleeding and has been shown to have lower mortality and less transfusion requirements than angiography. At the time of laparotomy, any obstetric issues can be concurrently addressed. If an arterial source of bleeding is suspected, angiography may be the more appropriate choice over laparotomy. The decision of whether to proceed first to laparotomy or angiography depends primarily on the clinical situation and institutional resources available.
Emergent cesarean section
If the fetus is viable and massive placental abruption resulting in nonreassuring fetal status or uterine rupture has occurred, the fetus should be rapidly delivered via cesarean section with a pediatric intensivist team ready to treat the neonate on delivery. In the setting of massive maternal hemorrhage and coagulopathy, hysterectomy may also need to be performed. In situations in which the mother has expired, a perimortem cesarean section should be performed emergently to save the life of a viable fetus. If cardiopulmonary resuscitation (CPR) is being performed for cardiac arrest, the treatment team must also immediately consider cesarean delivery. Perimortem cesarean section should be performed within 4 to 5 minutes of maternal cardiac arrest to increase the chances of both maternal and fetal survivability ; a review of the literature found that beyond 4 minutes of maternal CPR time, there is a low probability of fetal survival and a high probability of severe neurologic dysfunction if the fetus does survive. Perimortem cesarean section allows for better maternal perfusion with chest compressions once the mother’s abdomen is relieved of the gravid uterus.
Surgical considerations unique to the pregnant female
Surgical indications for pelvic and acetabular fractures are the same in pregnant women as in the general population. If surgery is indicated and the fetus remains viable through the acute stages of the trauma and resuscitation period, modifications to the standard surgical treatment of pelvic and acetabular fractures may be necessary to accommodate the fetus ( Fig. 1 ). If the fetus is not viable then surgical considerations are more straightforward and follow the standard of care for any pelvic or acetabular fracture once the patient is stabilized.
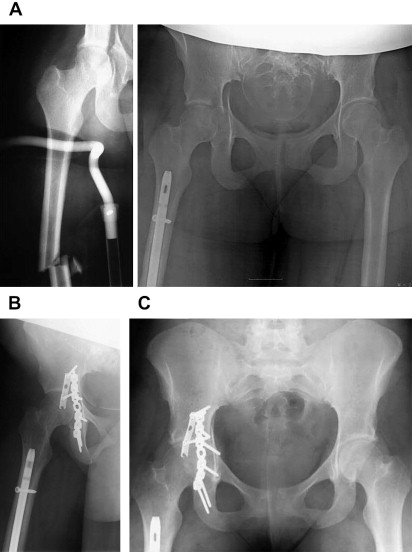
If the fetus is viable, modifications to the standard treatment include using external fixation only as the definitive treatment, assuming that the reduction and stability are adequate. This strategy avoids further insult to the surrounding uterine environment. Other options include using temporary skeletal traction with elective delivery of the fetus at a more advanced gestational age, followed by definitive operative treatment of the fracture. If possible, delivery should be delayed to at least 28 weeks’ gestational age to decrease the risks of immature lung development and intraventricular hemorrhage. Little benefit is seen by delaying delivery past 34 weeks of gestation. If a fetus is to be delivered before 34 weeks’ gestational age, antenatal steroids should be administered to aid in fetal lung maturity. In addition, if the fetus is less than 32 weeks’ gestational age, magnesium sulfate should be administered to help decrease rates of cerebral palsy. Postponing delivery for fetal benefit must be weighed against the risks of waiting to perform operative treatment of the mother. After 3 weeks after injury, it becomes more challenging to obtain an adequate reduction during pelvic and acetabular fracture surgery ; additional risks are related to long-term immobilization and bed rest, including aspiration, pulmonary embolus, and pressure ulcers. The risk of prolonged bed rest immobilization and the prognosis for posttraumatic deformity, early arthritis, and likelihood of needing future deformity correction surgery or arthroplasty should be discussed with the patient and family if delayed open reduction and internal fixation (ORIF) or nonoperative management is chosen. Alternatively, if the fetus is near term or full term, surgical fixation of the pubic symphysis can be performed at the same time as cesarean section via the same Pfannenstiel incision. In certain acetabular fracture patterns in which an anterior ilioinguinal approach is normally used, such as a transverse acetabular fracture, a posterior Kocher-Langenbeck incision may be used instead to stay on the outside of the pelvis and further away from the surrounding uterine environment. Although the goal of surgery is anatomic reduction of the pelvis or acetabulum, in pregnant patients, the aim may be a less than anatomic reduction to limit the length of the case, potential blood loss, and amount of radiation to the fetus. If less than an anatomic reduction is considered, the patient or her family should be counseled preoperatively about the increased risk of malunion, future progression to posttraumatic arthritis, and need for early arthroplasty.
Positioning in the pregnant patient
During surgery, the supine position should be avoided in the second and third trimesters in combination with general anesthesia, because it reduces cardiac output and can cause maternal hypotension and hypoxia to the placenta and fetus as a result of compression of the gravid uterus on the IVC. The left lateral decubitus position is ideal, because it takes the weight of the gravid uterus off the IVC and allows for better venous return and cardiac output. With respect to specific fracture patterns, alternatives to standard positioning may be elected. For instance, in a left posterior wall acetabular fracture, which is usually surgically fixed in the right lateral decubitus position, it would be safer to have the patient completely prone to take the weight of the uterus off the IVC. When the prone position is used, the abdomen and gravid uterus need to be carefully padded and free.
Intraoperative fetal monitoring in pelvic and acetabular surgery
There is significant controversy about the use of intraoperative fetal heart monitoring. The decision of whether or not to use it should be made on an individual basis in consultation with the obstetrics and anesthesia teams. If continuous fetal monitoring is used, an obstetrics team should be available in case emergent delivery is warranted. In case of emergency or signs of fetal distress, fetal monitoring equipment should be used when possible and an obstetrician available.
Anesthesia risks in the pregnant patient
An anesthesiologist experienced in obstetric anesthesia should be used. Modern general anesthesia in a pregnant woman is safe. Regional anesthesia reduces the risk of aspiration as well as the amount of systemic chemicals from general anesthesia to the mother and fetus; however, there is a risk of sympathetic blockade and hypotension, with resultant fetal hypoxia, more likely to occur with spinal than epidural anesthesia. Frequent blood pressure monitoring and in most cases an arterial line should be used to monitor for blood pressure fluctuations. In addition to the safety of the mother, the anesthesia team must consider risk of teratogenicity, fetal hypoxia, and preterm labor. Although most anesthetic agents are teratogenic in high doses in animal studies, they are considered safe in clinical practice. It is essential to avoid maternal hypotension, hypoxia, or major changes in physiologic acid-base levels of normal pregnancy to prevent fetal hypoxia. There is an increased risk of preterm labor postoperatively with abdominopelvic surgery. However, the risk of this complication is low, and prophylactic tocolytic therapy to inhibit contractions is generally not recommended because of its significant maternal side effects and unproved efficacy.
Radiation risks to the fetus
Pregnant patients undergoing trauma surgery are often concerned about the risk of radiation exposure on the developing fetus. So great are these fears that many women electively chose to terminate their pregnancy based on perceived risk of exposure. Patients should be counseled that most of these fears are unfounded. If the patient and family have questions or concerns regarding radiation exposure to the developing fetus, a radiation safety evaluation should be conducted to assess the amount of exposure and risk to the fetus so that the patient can make informed decisions.
Although studies of Japanese atomic bomb survivors have shown a dose-related correlation between prenatal exposure to ionizing radiation and teratogenesis, the doses required exceed any single diagnostic study. There is no association between fetal anomalies or demise with radiation doses of less than 5 rad (5 mGy) according to the American College of Obstetricians and Gynecologists and other radiation safety organizations. Major organ development occurs in the third to eighth week of gestation, and organ malformations can also be affected by high doses of radiation in this period. However, the risk of teratogenesis is greatest at 10 to 17 weeks of gestation (8–15 weeks after conception), a time of critical human brain development. Although carcinogenic risk, especially childhood leukemia, has been shown to be increased with as little as 1 to 2 rad of radiation exposure, the absolute risk of increase with this amount of exposure is extremely low, on the order of 1 in 10,000.
The risks of modern low-dose imaging techniques must be weighed against the risks of not having necessary and timely information to save the mother’s life and that of the fetus, as well as the risk of poor long-term function from a malunited pelvic ring or acetabulum. However, certain modifications can be made when considering radiation reduction exposure to the developing fetus. In acute trauma situations, all standard imaging studies should be obtained, which include anteroposterior view of the pelvis, lateral view of the cervical spine, and chest radiograph. Although some trauma centers have replaced the standard trauma radiographic series with a pan-scan, that is, a screening computed tomography (CT) scan of the entire body in polytrauma situations, this should be bypassed in known or suspected pregnancies ( Table 2 ).
| Radiographic Study | Rad | No. of Studies to Reach Cumulative 5 Rad |
|---|---|---|
| Cervical spine | 0.002 | 2500 |
| Chest (2 views) | 0.00007 | 71,429 |
| Pelvis | 0.040 | 125 |
| Hip (single view) | 0.213 | 23 |
| CT head (10 slices) | <0.050 | >100 |
| CT chest (10 slices) | <0.100 | >50 |
| CT abdomen (10 slices) | 2.600 | 1 |
| CT lumbar spine (5 slices) | 3.500 | 1 |
| Ventilation-perfusion scan | 0.215 | 23 |
The essential orthopedic radiographic studies are pelvic inlet and outlet views to characterize the fracture pattern in pelvic fractures or Judet views of the pelvis if there is an acetabular fracture. Although a CT scan is now the standard for examining for posterior pelvic ring involvement, sacral dysmorphism, or intra-acetabular fracture fragments, fracture pattern and morphology of the pelvis can almost always be diagnosed with plain radiographs alone. A pelvic CT scan (which conveys greater than the recommended maximum 5 rad amount to the fetus) should be bypassed to avoid high-dose radiation to the fetus. When a pelvic CT scan is deemed necessary by the treatment team, modifications of slice width and number have been described, which images only the areas of most interest to decrease the amount of radiation to the fetus.
An alternative to pelvic CT scan is magnetic resonance imaging (MRI). MRI/magnetic resonance venography (MRV) can be performed on preoperative patients with pelvic and acetabular fracture to diagnose pelvic vein thrombosis, and although not as specific as CT scan for assessing bone, it is usually adequate to assess for fracture pattern, intra-articular fragments, and sacral morphology. Furthermore, MRI has not been shown to have any deleterious effects on the developing fetus.
Intraoperatively, lead shielding of the uterus should be used if it does not interfere with imaging, and collimation of the image intensifier should be used to reduce exposure. Fluoroscopy should be used sparingly, and a more open approach than usual may be necessary to avoid relying heavily on intraoperative imaging. Furthermore, only the minimal amount of intraoperative fluoroscopy should be used to obtain the necessary intraoperative reduction. A carefully planned preoperative template should help the surgeon better understand the fracture and reduce the length of surgery and amount of intraoperative fluoroscopy.
Prophylaxis considerations for deep venous thrombosis and pulmonary embolism in pregnant women
The hypercoagulable states of pregnancy and trauma combined put the patient at high risk for developing deep venous thrombosis (DVT), so these patients should be placed on preventative doses of subcutaneous heparin or low-molecular-weight heparin once hemodynamically stabilized. These medications do not cross the placental barrier and are safe to use in pregnancy; warfarin is contraindicated in pregnancy because it crosses the placenta and enters fetal circulation. Mechanical prophylaxis with intermittent pneumatic compression devices should also be used. Preoperatively, screening Doppler ultrasonography should also be performed. Although an IVC filter is commonly used in patients with polytrauma with pelvic fractures, placement of the filter requires further radiation exposure and therefore is not indicated as a preventative measure. However, if a large-vein DVT is diagnosed by Doppler ultrasonography or MRV, an IVC filter may be indicated, because the risk of a fatal pulmonary embolus outweighs the risk of radiation to the fetus from IVC filter placement.
Summary
Pelvic fractures in pregnancy are life-threatening to both the mother and fetus. The priority of the trauma team should always be to the mother, because prompt treatment gives both the mother and the fetus the best chance for a favorable outcome. A multidisciplinary team approach should be used to address what are often complex and challenging cases and should involve input from general trauma surgery, orthopedics, obstetrics, pediatrics, obstetric anesthesia, and radiology as well as the patient and her family whenever possible. Modifications to the standard treatment of pelvic and acetabular fractures in pregnant women are often necessary with regards to anesthesia, radiation exposure, and surgery.
Pelvic ring trauma in the pregnant woman
Epidemiology of Trauma in Pregnancy
After primary obstetric causes, trauma is the leading cause of maternal death during pregnancy. Trauma occurs in approximately 7% of all pregnancies and is most often in conjunction with motor vehicle accidents (MVAs). Similar to the trauma-related mortality in nonpregnant women, the maternal mortality from trauma is approximately 10%, with the highest risk of maternal death occurring in the third trimester. Fetal death rates are significantly higher and have been reported to be as high as 50% to 65% in cases of severe trauma.
Fetal Morbidity and Mortality
Maternal death from trauma is associated both with fetal death and a high injury severity score. If the fetus survives the initial traumatic event, it is still at a higher risk of low birth weight, premature delivery, and permanent neurocognitive dysfunction than a pregnancy not affected by a traumatic event. Multiple case reports and series have identified associations between maternal trauma during pregnancy and cerebral palsy or developmental delay in the child. This brain injury is believed to be caused by a hypoxic insult to the developing fetal brain either from maternal hypotension or placental embolus at the time of the traumatic event.
The fetus is at greater risk of death caused by trauma than the mother. Fetal demise can be caused by direct trauma, preterm labor, maternal-fetal hemorrhage, placental abruption, or uterine rupture. Before 12 weeks of gestation, the fetus is contained entirely within the bony pelvis and is protected from direct trauma. However, after 12 weeks’ gestation, direct injury to the fetus can occur through the same mechanism as the pelvic fracture. Placental abruption is the most common complication of blunt trauma in pregnancy and is responsible for fetal death in 40% to 60% of trauma-related deaths versus 1% to 5% in nontraumatic causes of fetal death. It is theorized that the force of the traumatic event causes the elastic uterine lining to separate from the inelastic placenta, interrupting the gas exchange that occurs across the placental interface. If a complete placental abruption occurs, the fetus, if viable, must be delivered rapidly in order not to deprive the fetus of oxygenated blood. Even minor trauma can increase the risk of preterm labor, placental abruption, and fetal demise, especially if the abdomen or pelvis is involved.
Prevention Strategies
Because most severe trauma in pregnant women is caused by MVAs, the best evidence-based strategy to prevent related maternal and fetal morbidity and mortality is the use of safety belts. Approximately one-half of all fetal fatalities caused by MVAs are estimated to be preventable if seat belts are worn properly. The use of seat belts has been shown to reduce the rate of preterm labor and fetal demise in pregnant women involved in MVAs. Safety belts should have both a shoulder harness and lap belt. The lap belt should sit across the pelvic brim, not the gravid uterus, and the shoulder harness should rest between the breasts.
Epidemiology of Pelvic and Acetabular Fractures in Pregnancy
Few evidence-based studies have examined the outcomes of pregnant women who sustain pelvic fractures, because such cases are rare; however, 1 large population-based study found that pregnant women who sustain pelvic fractures were at high risk for placental abruption and fetal demise. A systematic review of the literature that reported on 101 total cases of pelvic or acetabular fractures in pregnant women found that although no single institution had significant experience with this combined patient-injury demographic, maternal and fetal death were more likely to occur with MVAs and pedestrians struck by a motor vehicle than with a fall. Mortality was not affected by fracture classification (simple or complex), type (pelvic or acetabular), pregnancy trimester, or study era. In this review, the fetal mortality was 35% and the maternal mortality was 9%, which is similar to mortality from high-energy trauma in general. In a 24-year study from a major European trauma center of 4196 patients with blunt polytrauma, only 7 of the patients who sustained a pelvic fracture were pregnant (0.17% incidence in the overall population of patients with polytrauma). The mean injury severity score of these 7 women was 29.9. Five of 7 mothers survived their injuries; however, only 3 of 7 fetuses survived, and 4 were found to be deceased at the scene of the accident. In 2 of the 3 mothers in whom the fetus survived, treatment was modified based on the viability of the fetus. In all 3 cases in which the fetus survived, the mother went on to uneventful delivery of the child without any long-term effects related to the mother’s injury. Almog and colleagues found that over a 15-year period, only 15 of 1345 patients who were treated at a trauma center for a pelvic or acetabular fracture were pregnant (1.1%). One woman died of her injuries and there were 4 cases of fetal death. Four of the 15 women underwent operative fixation of their fractures, and the rest were treated nonoperatively.
Acetabular fractures are considered part of the spectrum of injuries to the pelvic ring. Most studies that have reported on acetabular fractures in pregnant women are case reports; however, Porter and colleagues reported a case series of 8 pregnant women with acetabular fractures (of a total of 518 patients) who presented to a level I trauma center over a 6-year period. Gestational age in this group ranged from 5 to 26 weeks at the time of injury. All of the patients went on to deliver at at least 36 weeks with normal Apgar scores at delivery. Long-term follow-up on the children was not reported.
Evaluation and Treatment
Initial assessment
The most unique aspect of pregnancy-related trauma is that the trauma team must simultaneously address 2 patients: the mother and the fetus. Therefore, the treatment team should include not only the standard trauma team members but also a maternal-fetal medicine specialist. The priority in a pregnant trauma patient is timely treatment and resuscitation of the mother, because this leads to better outcomes for the fetus. Standard protocol of advanced trauma life support should be adhered to by addressing airway, breathing, circulation, disability, and exposure. All female trauma patients of childbearing age should have a rapid urine pregnancy test, because sometimes neither the patient nor the trauma team may be aware of an early pregnancy. Pelvic fractures caused by high-energy mechanisms are an indicator of severe polytrauma, and there is a high incidence of associated injuries, including head, thoracic, abdominal, and spinal injuries, some of which are immediately more life-threatening than the pelvic fracture itself.
Sources of blood loss, if not obvious on physical examination, should be discovered via chest radiograph, pelvic radiograph, and focused assessment with sonography in trauma (FAST) survey. A Foley catheter should be placed to monitor adequacy of resuscitation. The presence of blood at the vaginal introitus in a pregnant trauma patient should prompt the trauma and obstetric team to rule out placenta previa, placental abruption, or labor. Nonobstetric causes include urethral or bladder injury; if a nonobstetric cause is suspected, the patient should be evaluated by a urologist before Foley catheter placement. Blood at the vagina or rectum in the presence of a high-energy pelvic fracture may also indicate an open pelvic fracture, a diagnosis that carries a mortality of near 50% and requires operative debridement and stabilization once the patient is hemodynamically stable.
Fetal considerations in the acute setting
In any pregnant women beyond the threshold of viability, continuous fetal heart rate monitoring and a maternal tocometer to monitor for uterine contractions should be used in the acute setting. Depending on the center, fetuses are typically considered viable at 24 weeks’ gestational age; however, fetuses born at less than 30 weeks are at a significantly increased risk of cerebral palsy. In obtunded or intubated patients for whom no history is available, the location of the uterine fundus allows for a close estimate of gestational age, and in early pregnancies, the standard FAST scan may be diagnostic. On secondary survey, a pelvic examination should be performed by an obstetrician, who should look for bleeding, signs of labor, and cervical length or dilation. In the setting of a pelvic fracture, such an examination may need to be performed under sedation or general anesthesia because of pain or instability. In addition, a Kleihauer-Betke (KB) blood test, which detects fetal hemoglobin in maternal circulation, can aid in detecting occult maternal-fetal hemorrhage. It is unnecessary in obvious cases of severe trauma and maternal-fetal hemorrhage, but a positive KB test should prompt the treatment team to administer Rh immunoglobulin in all Rh-negative women.
Emergent reduction of the pelvis in the pregnant patient
If an open-book pelvic fracture (anteroposterior compression type) is diagnosed on examination or radiograph, and the patient is hemodynamically unstable, a pelvic sheet or binder should be placed to tamponade presumed bleeding from disrupted pelvic vessels. The pelvis can be close reduced by internally rotating the legs and compressing on the iliac wings when applying the sheet or binder. Internally rotating the legs and holding them together by taping the knees with cushioning between them is an assistive maneuver to hold the reduction. Military antishock trousers (MAST), although effective in keeping the pelvis reduced and creating a tamponade, are no longer recommended for treatment, because they limit access to the abdomen and cannot be used for any significant period out of concern for MAST-induced lower extremity compartment syndrome.
There are several unique aspects to closed reduction of the pregnant patient’s pelvis. The gravid uterus acts as a compressive device on the inferior vena cava (IVC) when the pregnant patient is supine, which inhibits venous return and decreases cardiac output. Close reducing an open-book pelvic fracture with a sheet or a binder may worsen this problem by increasing the compression of the gravid uterus on the IVC, further decreasing venous return to the heart and cardiac output. Certain measures may help to mitigate this problem once the pelvic binder or sheet is placed. If the patient is too unstable to be placed into the full left lateral decubitus position or if there is a concurrent spinal injury preventing safe left lateral decubitus positioning, a roll or wedge may be placed under the right side of the backboard in spinal immobilized patients, or the bed rotated with the right side up. This left lateral tilt position mechanically allows the uterus to fall to the left, relieving some pressure on the compressed IVC and improving venous return to the heart and improving cardiac output by as much as 30%. There is little clinical evidence to support what degree of tilt to use ; however, the general recommendation is that 15° of left lateral tilt is acceptable. Another maneuver that may help take pressure off the IVC is for an experienced obstetrician to manually shift the gravid uterus to the left of the abdomen.
Resuscitation measures specific to a pregnant woman
Many physiologic changes during pregnancy occur and must be considered during resuscitation ( Box 1 , Table 1 ). After 20 weeks of gestation, the pregnant woman’s plasma volume is significantly increased and up to 1500 mL of blood loss can occur before hemodynamic instability becomes apparent. About 50% more fluid than usual may be required before improvement in hemodynamic status is observed. The treatment team should be aware of certain normal laboratory values in pregnant women; for instance, the normal arterial P co 2 (partial pressure of carbon dioxide) level is less than a nonpregnant patient, and if a pregnant patient’s value is in the normal nonpregnant range, hypoxia is present. If the mother’s blood type is not known, all blood products administered acutely should be Rh-negative to prevent a fetal transfusion reaction and Rh immunoglobulin should be administered. Moreover, a secondary coagulopathy or acute hypoxic event can occur as a result of amniotic fluid embolus.
Related posts:
 Results and Outcomes of Unicompartmental Knee Arthroplasty
Technical Pitfalls of Shoulder Hemiarthroplasty for Fracture Management
Posterior Elbow Wounds
Management of Radial Nerve Palsy Following Fractures of the Humerus
Technical Pitfalls of Shoulder Hemiarthroplasty for Fracture Management
Reverse Shoulder Arthroplasty
Results and Outcomes of Unicompartmental Knee Arthroplasty
Technical Pitfalls of Shoulder Hemiarthroplasty for Fracture Management
Posterior Elbow Wounds
Management of Radial Nerve Palsy Following Fractures of the Humerus
Technical Pitfalls of Shoulder Hemiarthroplasty for Fracture Management
Reverse Shoulder Arthroplasty
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


