Management of Olecranon Nonunion
Bernard F. Morrey
INTRODUCTION
Even with careful attention to the principles described earlier, nonunion may occur with a reported incidence of up to 5%. There are two types of olecranon nonunions with significant difference in management: undisplaced and displaced. The treatment of nonunion follows principles of primary fracture treatment and therefore depends entirely on the type as classified earlier. Although the blood supply and vascularity of the cancellous olecranon are felt to be sufficient without bone grafting when reconstruction for nonunion is carried out, the authors use routine iliac inlay or onlay grafting.
The following factors determine the treatment options for olecranon nonunion:
When nonunion occurs in the proximal 50% of the olecranon, excision is an acceptable alternative and is the treatment of choice in the elderly or osteoporotic patient.
If there is no gross deformity the inlay bone plug technique is used.
For gross deformity, rigid low-profile dynamic compression plating (LDCP) plate fixation with or without an intramedullary screw but always with an onlay corticocancellous “bone plate” is the preferred strategy (1).
UNDISPLACED, SYMPTOMATIC NONUNION
Lateral Inlay Plug Bone Graft
For minimally displaced nonunion this technique has worked well. Incision and exposure are identical to those used for the acute fracture, with the exception of the patient being positioned in the prone posture with the arm over a padded armrest to permit use of a fluoroscopic C-arm. This position is chosen to permit ease of obtaining a better corticocancellous graft from the posterior rather than the anterior iliac crest. Care should also be taken to carefully identify and protect the ulnar nerve (Fig. 4-1). Any previously placed metal is removed and the area of pseudarthrosis is identified through the periosteum.
The pseudarthrosis is debrided of fibrous tissue to viable bone with a rongeur, curette, and motorized bur, avoiding the removal of any vascularized bone (Fig. 4-2).
Using a 7/16-inch Cloward circular plug cutter, corticocancellous plugs of bone (additional in case of loss) are taken from the posterior iliac crest (Fig. 4-3), and an additional piece of cancellous bone is cut to fit the pseudarthrosis defect in the olecranon at the site of nonunion.
Large AO 6.5-mm intramedullary screw and tension band wire fixation is carried out as described earlier. Particular care is taken to avoid any change in the normal contour of the sigmoid notch as compression is accomplished with the compression screw.
A corresponding 7/16-inch Cloward circular cutting drill is then used to make a hole at the site of olecranon pseudarthrosis laterally (Fig. 4-4), and the previously harvested plug of iliac graft is tapped into the prepared hole (Fig. 4-5). Additional small fragments of cancellous bone graft may be placed in any irregularity in the pseudarthrosis site.
The wires and the intramedullary screw are tightened.
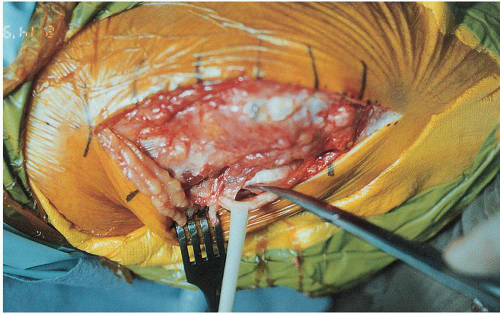 FIGURE 4-1 Because exposing nonunions is typically more difficult, particular care should be made to identify the ulnar nerve to avoid injury. |
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


