Lumbar Microdiskectomy
Patient Selection
Indications
Patients present with leg pain, or “sciatica,” that follows radicular pattern
Thorough history and physical examination can predict level of IDH before confirmatory imaging studies
Strongest indication—Progressive loss of motor function (eg, footdrop) interfering with quality of life
Most common indication—Intractable pain despite nonsurgical treatment
Contraindications
No evidence of IDH present on imaging studies
Pay attention to patients with painless footdrop; differential diagnosis extensive; consider peroneal nerve palsy, tertiary syphilis, diabetic mononeuropathy, fascioscapulohumeral dystrophy, stroke, multiple sclerosis, and amyotrophic lateral sclerosis when paucity of findings present on MRI
Greater trochanteric pain syndrome commonly causes radiating leg pain; can mimic L5 radiculopathy (pain in gluteus and lateral thigh); not characterized by radiation of pain below proximal calf
Preoperative Imaging
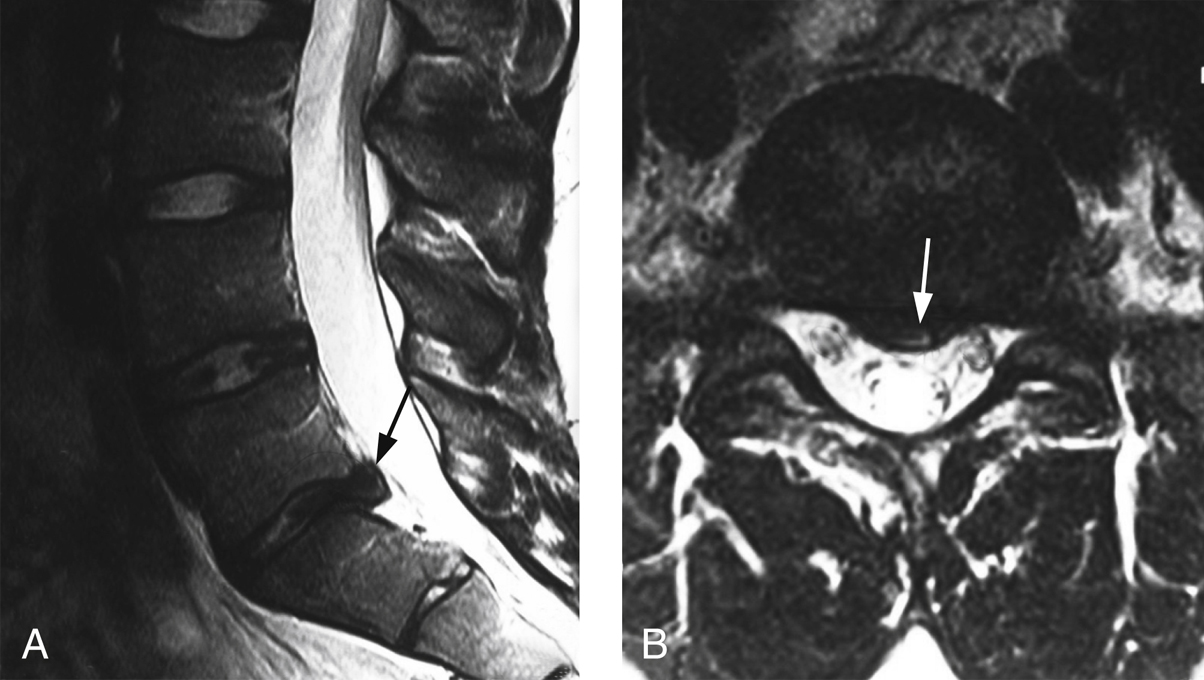
Figure 1T2-weighted MRIs show the spine of a 21-year-old athlete with left S1 radiculopathy. A, Sagittal image demonstrates an L5/S1 disk herniation (arrow). B, Axial image demonstrates the left paramedian location (arrow).
Closed MRI gold standard for identifying suspected herniated nucleus pulposus (HNP)
Sagittal T2-weighted sequences (Figure 1, A) identify level and degree of foraminal encroachment
Axial T2-weighted sequences (Figure 1, B) determine whether HNP is central, paramedian, subarticular, or far lateral; in far-lateral HNP, axial T1-weighted images may better show HNP because high-signal-intensity fat outside canal contrasts with low-signal-intensity disk material
Obtain plain radiographs before surgery to evaluate for deformity (scoliosis or spondylolisthesis) or spina bifida occulta (may not show on MRI obtained in supine position)
Procedure
Room Setup/Patient Positioning
Prone position on Jackson table; pad bony prominences well
Suspend face and head in padded holder; enables clear visualization of eyes, nose, and endotracheal tube
Flex knees; pad legs with memory foam pillows
Bring table into jackknife position; reduces lumbar lordosis and facilitates exposure of disk by increasing interlaminar distance
Bring C-arm into lateral position; drape out of sterile field after preparing skin
Special Instruments/Equipment/Implants
C-arm fluoroscope
Surgical microscope
Adjustable Jackson table
Surgical Technique for Lumbar Microdiskectomy
 | Video 104.1 Lumbar Microdiskectomy. Bradley Moatz, MD; P. Justin Tortolani, MD (30 min) |
Preparation
Palpate iliac crest on sides of patient; serves as guide to L4 vertebral level
Insert spinal needle off midline, directed toward disk of interest; obtain lateral fluoroscopic image to visualize marker, confirming best location for skin incision
Exposure


Figure 3Intraoperative lateral fluoroscopic image shows the lumbar spine after the Taylor retractor has been positioned around the lateral aspect of the L5-S1 facet joint. The tip of the Taylor retractor points to the level of the diskectomy. A Penfield 4 is placed along the posterior aspect of the L5-S1 as a final confirmation of the desired surgical level.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


