Clinicians must have knowledge of the growth and development of the adolescent spine and the subsequent injury patterns and other spinal conditions common in the adolescent athlete. The management and treatment of spinal injuries in adolescent athletes require a coordinated effort between the clinician, patients, parents/guardians, coaches, therapists, and athletic trainers. Treatment should not only help alleviate the current symptoms but also address flexibility and muscle imbalances to prevent future injuries by recognizing and addressing risk factors. Return to sport should be a gradual process once the pain has resolved and the athlete has regained full strength.
Key points
- •
Low back pain is frequently encountered in adolescent athletes.
- •
The adolescent athlete is at risk for significant structural injuries as well as nonmechanical problems.
- •
Adolescent athletes who present with low back pain are more likely to have structural injuries and therefore should be investigated fully.
- •
Any athlete with severe, persisting, or activity-limiting symptoms needs to be evaluated thoroughly.
- •
It is imperative to complete a comprehensive evaluation of back pain, and a cause such as muscle strain should be a diagnosis of exclusion.
Introduction
Low back pain is a common problem among adolescent athletes. It is estimated to occur in 10% to 15% of young athletes, but the prevalence may be higher in certain sports. Back pain has been reported as high as 27% in football and between 50% and 86% in gymnastics. Although adolescent athletes are undergoing their pubescent changes into adulthood, they cannot be treated like young adults. Therefore, the approach to the treatment of adolescent athletes with low back pain can be difficult and requires thorough understanding of spinal development.
The demographics of adolescents with low back pain varies from that of adulthood, Although there are many conditions that occur in both adolescence and adulthood, there are certain spinal disease/injury processes that are unique to the growing adolescent spine. One of the key factors to consider in the adolescent athlete is the ongoing growth and development of the adolescent spine. The growing spine introduces variables into the assessment and management of injuries to the spine that do not exist in the mature and developed spine of the adult population. For example, injuries of the pars interarticularis are more common in the adolescent spine, occurring in up to 47% of young athletes, whereas disk-related problems are uncommon in children; only 11% of children have disk-related disease, compared with 48% of adults. Idiopathic pain is also less common in young athletes. Physicians who attribute low back pain in young athletes to simple back strains, without investigations, run the risk of delaying the diagnosis and appropriate treatment of more serious injuries, such as spondylolysis or spondylolisthesis. Therefore, it is imperative that the clinician is aware the development of the spine and subsequent variances in injury patterns and frequencies when evaluating the adolescent athlete.
In addition to the structural considerations of the spine, the clinician should also be aware of potential physiologic, psychological, social, and cultural issues that may exist and affect the approach to diagnosis and management of adolescent spine disorders. To treat these athletes appropriately, clinicians need to develop a relationship with the athlete’s parents/guardians, coaches, and other potential athletic support staff to facilitate compliance with the activity modifications and treatment necessary to provide optimal rehabilitation to the injured spine. The coordination of care with the athlete’s support team facilitates the athlete’s recovery, training, and performance.
Introduction
Low back pain is a common problem among adolescent athletes. It is estimated to occur in 10% to 15% of young athletes, but the prevalence may be higher in certain sports. Back pain has been reported as high as 27% in football and between 50% and 86% in gymnastics. Although adolescent athletes are undergoing their pubescent changes into adulthood, they cannot be treated like young adults. Therefore, the approach to the treatment of adolescent athletes with low back pain can be difficult and requires thorough understanding of spinal development.
The demographics of adolescents with low back pain varies from that of adulthood, Although there are many conditions that occur in both adolescence and adulthood, there are certain spinal disease/injury processes that are unique to the growing adolescent spine. One of the key factors to consider in the adolescent athlete is the ongoing growth and development of the adolescent spine. The growing spine introduces variables into the assessment and management of injuries to the spine that do not exist in the mature and developed spine of the adult population. For example, injuries of the pars interarticularis are more common in the adolescent spine, occurring in up to 47% of young athletes, whereas disk-related problems are uncommon in children; only 11% of children have disk-related disease, compared with 48% of adults. Idiopathic pain is also less common in young athletes. Physicians who attribute low back pain in young athletes to simple back strains, without investigations, run the risk of delaying the diagnosis and appropriate treatment of more serious injuries, such as spondylolysis or spondylolisthesis. Therefore, it is imperative that the clinician is aware the development of the spine and subsequent variances in injury patterns and frequencies when evaluating the adolescent athlete.
In addition to the structural considerations of the spine, the clinician should also be aware of potential physiologic, psychological, social, and cultural issues that may exist and affect the approach to diagnosis and management of adolescent spine disorders. To treat these athletes appropriately, clinicians need to develop a relationship with the athlete’s parents/guardians, coaches, and other potential athletic support staff to facilitate compliance with the activity modifications and treatment necessary to provide optimal rehabilitation to the injured spine. The coordination of care with the athlete’s support team facilitates the athlete’s recovery, training, and performance.
Growth and development of the spine
There are distinct structural differences of the spine in adolescents from the adult spine, which affect the nature of injury. Compared with the adult spine, the relatively greater hydrophilic nature of the nucleus pulposus of the spine of a child allows for more effective force absorption and central distribution of force transfer to the adjacent vertebrae. However, the composition of the nucleus pulposus begins to change as early as 7 or 8 years old, resulting in a more peripheral force distribution of the disk. There are 3 primary ossification centers of the vertebrae: one in the vertebral body and 2 in the vertebral arch. The 2 ossifications in the center of the vertebral arch typically fuse by 2 to 6 years, and spinal bifida occulta results, caused by failure of fusion of these primary centers. Pars interarticularis defects/fractures are more common in the adolescent spine, occurring in up to 47% of young athletes, and are postulated to be caused by incomplete bony maturation present in the neural arch. Biomechanical studies have indicated that the bony strength of the vertebrae, particularly the neural arch, can increase into the fourth or fifth decade of life.
The physes associated with the vertebral end plates facilitate the growth of the vertebral body. Hyaline cartilage adjacent to the nucleus pulposus and physeal cartilage adjacent to the vertebral body comprise the vertebral end plate. A ring apophysis and an end-plate physis comprise the physeal cartilage. The growth of the vertebral body is facilitated by the ring apophysis, which surrounds the periphery of the vertebral body and begins to ossify at 7 or 8 years old, whereas vertical growth of the vertebral body is caused by end-plate physis, which begins to fuse with the vertebral body at about age 14 to 15 years, with final closure occurring around age 21 to 25 years.
In addition to understanding the structural aspects of the growing adolescent spine, the clinician needs to be familiar with the variances of pubescent spinal development to assist in the diagnosis and management of spinal injuries. Schmorl nodes occur more frequently in children and adolescents compared with adults. Schmorl nodes are vertebral end-plate herniations of disk material, which are postulated to result from a combination of more central distribution of force via the nucleus pulposus combined with a relatively weak vertebral end plate. The adolescent athlete is also at increased risk for apophyseal ring fractures during the ongoing physeal development until ossification.
Another significant variation in injury patterns related to spinal development is disk-related disease in comparing the growing adolescent with mature adults, with the incidence at 11% in children compared with 48% in adults. The proposed pathophysiologic basis for this significant age-related variance is the relative strength of the intervertebral disk compared with that of the adjacent bone in adolescents compared with those in adults.
There is a significant variance in individual adolescents in the onset of puberty and the subsequent rate of growth and maturation. The variance between adolescents results in significant differences in size, strength, and skeletal maturity among children of the same chronologic age. Children between 6 and 10 years of age grow about 5 to 8 cm per year and gain about 2 to 3 kg per year. During adolescence, the growth rate increases, leading first to increases in height followed by increases in weight. On average, girls enter adolescent growth spurt and reach their maximal growth velocity about 2 years before boys. Weight gain occurs during the maximal growth in height, with girls gaining about 7 kg in fat-free mass, whereas boys gain about twice this amount.
Demographics
Although low back pain commonly occurs in the adolescent population, adolescent athletes who participate in specific sports such as football or gymnastics may be at a more substantial risk of pain and structural injury than others at the same chronologic age. The overall lifetime prevalence of low back pain by the midteenage years has been found to be 50% or greater in general population studies, with 1-year prevalence rates of 17% to 50%. In several studies, an increase in the prevalence of low back pain with age throughout childhood has been reported, with some of these studies also reporting higher rates of spinal injuries in girls than boys. A definitive connection has yet to be established between physical activity and low back pain, because the previous studies have had a significant variance in their results. In an attempt to provide more objective evidence with the use of an accelerometer to assess activity levels in children and adolescents, Wedderkopp and colleagues did not find any association between physical activity and low back pain. However, several studies have identified an association in adolescents with low back pain between depression and other emotional problems. Another significant risk factor showing a strong correlation was that the development of low back pain during adolescence increased the likelihood for the development of low back pain as an adult in a large-scale twin study.
There is a significant variance in the incidence and the specific spinal pathologic injury in adolescent athletes depending on the specific sport and also the position in a given sport. Contact sports such as football and rugby have a significantly higher incidence of acute injuries from high-energy impacts. In comparison, there is a greater incidence of overuse injuries with sports requiring repetitive flexion, extension, and torsion, such as gymnastics, figure skating, and rowing. A significantly higher rate of low back pain in a group of female gymnasts and figure skaters and male hockey and soccer players compared with nonathletes has been noted (45% vs 18% over 3 years). However, low back pain spans most sports in the adolescent population and was found to be a significant problem in golfers, rowers, and rugby players.
Gymnasts in particular have shown a significantly high incidence of spinal injury (between 50% and 86%) in several studies. These findings are limited not only to female gymnasts, because another study of male gymnasts showed that 79% of the male gymnasts had low back pain compared with 38% of their controls. In another study assessing wrestlers, gymnasts, and soccer and tennis players, 65% of these athletes had a history of low back pain, with male gymnasts having the highest frequency, at 85%.
Radiologic findings
There have been numerous studies regarding the incidence of radiologic findings in adolescent athletes. The results of these studies have shown that there are high rates of structural abnormalities on imaging studies of adolescent athletes in specific sports. As noted earlier, there was an increased incidence of low back pain symptoms in adolescent athletes who participate in gymnastics, and this trend also continues in the radiologic evaluation of their spines. In a study on the incidence of findings of back pain in male gymnasts, magnetic resonance imaging (MRI) showed statistically significant differences in spinal diseases in gymnasts compared with controls, with findings of thoracolumbar disk degeneration (75% compared with 31%), Schmorl nodes (71% compared with 44%), and injuries to the ring apophysis (17% compared with 0%). These findings were also shown in another study by Goldstein and colleagues, who reported higher rates of various structural abnormalities on MRI studies of elite gymnasts compared with elite swimmers. Another study by Bennett and colleagues performed MRI of the spine of elite female gymnasts, showing apophyseal injuries in almost half and disk degeneration in more than 60%.
Radiographic findings of spinal disease are not limited to adolescent gymnasts. Structural abnormalities on plain radiographs were shown in greater than 60% of the high-school and collegiate football players and in 74% of the rugby players assessed in 2 separate studies by Iwamoto and colleagues. Several studies have also shown higher rates of spondylolysis in high-level adolescent athletes participating in a variety of sports compared with nonathlete adolescents in the general population. Despite high levels of structural abnormalities on plain films and high rates of reported low back pain for young athletes competing in several sports, longer term follow-up studies on many of these athletes did not show any significant increased risk for ongoing low back pain into adulthood compared with the general population.
Considerations in the evaluation of low back pain in the adolescent athlete
Injuries to the low back may be caused by an acute traumatic event; however, they are more frequently secondary to overuse injuries caused by chronic repetitive microtrauma. It is imperative to complete a thorough assessment of all adolescent athletes who report symptoms of low back pain to evaluate for the presence of spinal disease. As noted earlier, because of the ongoing growth and development of the adolescent spine, the incidence of specific spinal diseases in adolescent athletes varies from adults. The clinician should also be cognizant of potential nonmechanical causes of low back pain, such as neoplasms, infection, developmental disorders, and systemic inflammatory rheumatisms. One must formulate a strong differential diagnosis and subsequently through the evaluation process develop a rational diagnostic strategy based on a thorough history, review of systems, and physical examination. The clinician should always inquire about any potential red flag symptoms, such as unexplained weight loss, pain at night, pain with recumbency, progressive neurologic deficits, and any loss of bowel or bladder function. In addition, one should inquire about any additional symptoms during a review of symptoms, which may show a systemic process, such as a rheumatic disorder.
Risk factors
As the adolescent athlete undergoes pubescent changes leading to periods of rapid growth, the muscles and ligaments are unable to maintain the pace of the rate of bone growth. This discrepancy places the adolescent athlete at greater risk of injury, as a result of muscle imbalance and a decrease in flexibility. The skeletally immature spine of adolescent athletes is also vulnerable to injury of the growth cartilage and secondary ossifications centers, because these areas are the weakest link of force transfer and are susceptible to compression, distraction, and torsion injury.
The vertebral bodies and intervertebral disks comprise the anterior column of the lumbar spine. Epiphyseal growth plates are located at both ends of the vertebral bodies and have overlying cartilaginous growth plates and ring apophyses, which attach to the outer annulus fibrosus. Repetitive flexion may lead to intervertebral disk herniation through the ring apophysis, a secondary ossification center, and injury to the ring apophysis can result in avulsion fractures.
The facet joints, spinous process, and pars interarticularis make up the posterior column of the lumbar spine. Ossification of the posterior column of the spine progresses from anterior to posterior and may be congenitally incomplete in the area of the superior portion of the pars interarticularis of the lower lumbar vertebrae, particularly at the L5 level, predisposing to spondylolytic stress fractures. The presence of spina bifida occulta at the lumbosacral junction seems to be an additional risk factor for spondylolysis. Traction from the dorsolumbar fascia and lordotic impingement may affect the growth cartilage of the facet joint and spinous process apophysis of the posterior arch.
Because of the considerable variance in the timing and tempo of growth among children, smaller, less mature athletes may be at higher risk for injury from contact from larger athletes, particularly in contact sports.
Several potential risk factors for spinal injury or low back pain in athletes have been identified. These factors include previous low back or lower extremity injuries, incomplete rehabilitation of previous injuries, decreased endurance, lower extremity muscle imbalance, high number of hours of participation per week, and the occurrence of stressful life events. Additional proximate causal factors associated with sports-related injury may include the individual mechanics and skill level associated with sports performance, training patterns, and equipment or facility problems.
Training volume and intensity can also cause injuries, particularly when young athletes participate in a sport for longer periods, such as at tournaments and sports camps. However, it is difficult to determine the appropriate amount of training for adolescent athletes, because of the variance in toleration of similar volumes of training. Overuse injuries present more often in athletes experiencing rapid growth, suggesting that the volume and intensity of training that an athlete’s body can tolerate vary as the athletes grow and mature.
Poor technique, abdominal muscle weakness, hip flexor/hamstring/thoracolumbar fascia tightness, increased femoral anteversion, genu recurvatum, and increased thoracic kyphosis serve as additional risk factors for low back pain. These factors add additional stress to the posterior elements of the spine as a result of increased lumbar lordosis.
Prevention
Although injuries are a part of sport, there are ways to reduce the risk of injury in young athletes. Recognizing risk factors is a key component to reducing injury. Before the start of a sport season, a preparticipation evaluation may identify certain risk factors, such as previous injuries that have not been fully rehabilitated or muscle weaknesses or inflexibility. These areas can then be addressed before the start of the season. In addition, athletes should start general strength and fitness conditioning several weeks before the start of the season. Increases in the frequency and intensity of training should be gradual, to allow for safe adaptation to the demands of the sport.
During periods of growth, young athletes are prone to loss of flexibility and muscle imbalances, which can predispose them to injury. Because of this concern, young athletes should reduce the amount of training and the volume of repetitive motions during growth spurts. Certain sports require maneuvers that place a lot of stress on the posterior spine, such as layback spins in figure skating and walkovers in gymnastics. Athletes may need to limit the number of repetitions of these maneuvers, particularly if pain is associated with these maneuvers. Core strengthening exercises and stretches for tight hamstrings and hip flexors may help reduce the risk of low back pain.
Proper technique should be emphasized in all athletes. It is important to correct posture to limit the amount of lordosis of the lumbar spine, which can help prevent injuries to the lumbar spine. In sports requiring lifting, such as pairs skating and dance, proper lifting techniques must be used to prevent back injuries.
In team sports, there can be large discrepancies in the sizes and relative strengths of participants on any given team. Attempts should be made to match athletes in size and strength to prevent injuries from contact with larger, stronger participants.
Another important aspect of prevention is recognizing that back pain is not part of the sport. Increasing complaints of pain, particularly if it is interfering with activity, should be taken seriously and addressed early to avoid significant injury.
History and physical examination
A comprehensive history is an essential initial step in the evaluation of adolescent athletes with low back pain. The mode of onset, location, quality, severity, and progression over time of the individual’s symptoms provide useful insight into potential causes. Symptoms that remain mild for an extended period before presentation may be suggestive of less significant structural injuries or more indolent underlying processes, whereas more severe, acute, or progressive symptoms may suggest a more substantial structural injury or a rapidly progressive process, such as infection. In addition, the provider should inquire about back pain eliciting any neurologic symptoms and aggravating factors.
The nature of an athlete’s specific sport and the position played may also predispose that individual to particular problems as well as the volume of training and level of competition. The timing of injury or pain in relation to the competitive season or training cycle may be relevant for both diagnosis and treatment. It is also important to inquire if there have been any recent increases in the training volume or intensity of the athlete. Thorough review of the dietary history, previous injuries, and the menstrual history of female athletes is also of importance.
Primary importance should be placed on the potential of red flag symptoms, such as fever, malaise, unexplained weight loss, pain at night, morning stiffness, bowel or bladder incontinence, and progressive neurologic weakness. Pain at night is often believed to be suggestive of an infectious or neoplastic process. Fever, lethargy, weight loss, rashes, headaches, and similar symptoms raise concern for significant systemic processes, including infection and malignancy. Morning stiffness or additional joint symptoms may suggest a diffuse inflammatory process. A past history or family history of HLA-B27-associated conditions, such as psoriatic arthritis, ankylosing spondylitis, reactive (Reiter) arthritis, or inflammatory bowel disease, may help in determining systemic causes of low back pain.
Isolated axial low back pain without lower extremity symptoms should be viewed differently from a presentation that includes leg pain or neurologic dysfunction, such as numbness, tingling, weakness, or changes in the bowel or bladder. Radicular symptoms such as radiation of pain down the leg and motor or sensory changes suggest the presence of nerve root or cord involvement. Bilateral leg pain suggests bilateral foraminal involvement and should expand the clinician’s differential diagnosis. At this point, one should consider and make specific assessment to help differentiate between a significant spondylolisthesis, central canal stenosis, disk herniation in the setting of a congenitally small spinal canal, or a cord process. The presence of lower extremity symptoms does not always mean that they are of spinal origin, and the clinician should also assess for other concomitant nonspinal diseases such as stress fractures, compartment syndrome, or other musculotendinous injuries. The location of the back pain can also significantly affect the differential diagnosis. Thoracic or thoracolumbar pain may be associated with diskogenic processes or Scheuermann kyphosis. Low lumbar pain has many potential causes, including disk disease, central or foraminal stenosis, spondyloarthropathies, and myofascial pain. Pain in the sacral or gluteal region may be more associated with conditions such as sacroiliitis or a sacral stress fracture; however, one still must assess for referred pain from the lumbar facets or nerve root involvement.
After the completion of a thorough history of present illness, the clinician should perform a comprehensive physical examination. The physical examination should be structured to identify significant and specific conditions that were formulated on the differential diagnosis. The result of a thorough history and physical examination should develop a strategic plan of further diagnostic and treatment options.
The physical examination should always be thorough, including inspection of any structural imbalances or asymmetries, lumbar range of motion, lumbosacral and pelvic motion, palpation of the spine, lumbar paraspinals, sacroiliac (SI)/pelvic muscles and joints, and a neurologic examination. It is important to assess lower extremity alignment and function, balance, and spine-specific provocative maneuvers. Gait assessment should be performed to assess for abnormalities such as antalgia, ataxia, or Trendelenberg gait.
The examiner should observe the athlete’s spine by having the patient wear a gown open to the back. When observing the athlete from behind it is important in the spine, shoulders, and pelvis to identify that the bony and soft tissue structures on both sides of the midline are symmetric. Visual inspection of the spine should evaluate for the presence of any abnormalities such as hemangiomas, café-au-lait spots, hairy patches, or skin dimples that may indicate spinal disease. Inspection should also identify any abnormal curvatures of the spine, such as scoliosis, excessive kyphosis, or lordosis.
Range of motion of the spine should be assessed in flexion, extension, rotation, and lateral flexion (bending). Adolescent athletes should be able to complete forward flexion of the spine and come close to touching their toes without knee flexion. Caution must be used to identify limitation of this motion because of tight hamstrings. Pain with flexion is suggestive of injury to the anterior spinal elements or lumbar muscle strain/spasms. The posterior elements of the spine can be assessed with hyperextension and facet loading (hyperextension with rotation).
Palpation for tenderness of the spine, lumbar paraspinals, and the SI joint is an integral part of the spinal assessment. Myofascial trigger points are taut, palpable bands in the lumbar paraspinal and gluteal muscles, which elicit or trigger the athlete’s pain. Tenderness of the SI joint has a positive predictive value for SI disorder.
Special tests include tests for the SI iliac joints, facet joints, and neural tension signs. These tests include FABER (flexion-abduction-external rotation), Gaenslen sign, Gillet test, seated slump test, straight leg raise, Lasègue maneuver, Bragard sign, Lazarević sign, and facet loading.
Additional assessment should be completed to assess the hip to rule out hip disease as well as the abdomen to rule out visceral disease. In female athletes, a pelvic examination may be warranted, particularly if menstrual abnormalities are reported by the patient during the history. The neurologic examination should include assessment of motor strength, sensation, and deep tendon reflexes of the lower extremities.
Clearly, other components of a comprehensive physical examination need to be included as medically appropriate, as well. Consideration does need to be given to the potential for significant structural injury, including fracture, and the examination should always be modified appropriately for a given patient to elicit essential information and avoid further harm.
Radiographic evaluation of the adolescent spine
Spinal imaging should be considered as an additional diagnostic option to assist in establishing a specific diagnosis. There are a variety of different imaging modalities to assist in the diagnostic evaluation, and clinicians need to be familiar with the each of their strengths and limitations. In addition, the clinician should be comfortable with directly assessing the images. Given the relative sensitivities and specificities of the various diagnostic options, the clinician should develop a plan for which imaging modality would provide the most appropriate objective findings based on the formulated differential diagnosis. In addition, the clinician should also consider that the amount of exposure to radiation in the adolescent athlete is of particular concern. Therefore, specific radiographic options should include the risk assessment of radiation exposure versus the potential comparative benefit of the various diagnostic options. The imaging strategies vary based on clinical concerns of the presenting symptoms and findings during the history and physical examination and are discussed in greater detail with each specific spinal condition.
Special considerations in the adolescent athlete
Treatment of adolescent athletes involves several specific considerations, as well. The state and demands of physiologic development of the athlete need to be taken into consideration when planning physical training. The psychosocial environment of an injured athlete may also pose challenges for treatment, and the psychological impact of injury can be difficult for athletes and their families. The use of medications may be problematic, as well. There are limited to no data on the effects on children and adolescents of several different medications commonly used to manage pain in adults. Care needs to be taken regarding weight and age in prescribing medications to young athletes, and clinicians need to be aware of any potential conflicts with substance use policies that may apply to an athlete’s given sport or level of competition. There are also high rates of use of ergogenic aids and performance-enhancing supplements among adolescent athletes, which introduce the potential for medication interactions, among other problems. The use of these supplements, legal or illegal, may not necessarily be reported to clinicians routinely, and the likelihood of this seems even lower if specific questions regarding their use are not asked.
Specific spinal conditions and injuries
There are several specific clinical entities that are particularly important to understand in managing young athletes with low back pain. These entities include spondylolysis, spondylolisthesis, posterior element overuse syndrome, diskogenic injuries, vertebral body apophyseal avulsion fracture, Scheuermann kyphosis, SI pain, and other causes of low back pain. These individual conditions are discussed in greater detail in the following sections.
Spondylolysis and Spondylolisthesis
Spondylolysis is a common cause of spinal disease in the adolescent spine and should be considered as a diagnostic possibility in almost every adolescent athlete with significant low back pain. However, it should be high on the differential diagnosis in all athletes who compete in sports involving repetitive extension and rotation, such as gymnastics, figure skating, and rowing. Spondylolysis is definitively the most frequent diagnosis (47%) made in adolescent athletes presenting with low back pain.
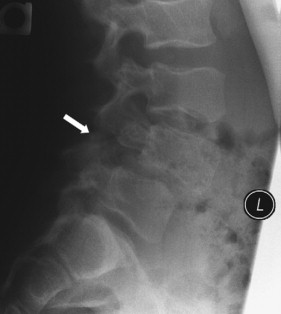
Spondylolysis refers to a defect in the pars interarticularis of the vertebral arch, a stress fracture caused by repetitive extension and torsion of the spine, and is most common at L5 and on the left side. Bilateral spondylolysis at the same vertebral level can result in spondylolisthesis. Spondylolisthesis is a separate but related term referring to the anterior displacement of a vertebral body compared with its alignment with the adjacent vertebral body ( Fig. 1 ). Spondylolisthesis is graded using the Meyerding scale according to the percentage of slip: grade 1 is a slip of 0% to 25%, grade 2 is 25% to 50%, grade 3 is 50% to 75%, grade 4 is 75% to 100%, and grade 5 is more than 100%.
Spondylolysis and spondylolisthesis are most frequently viewed under the categorization proposed by Wiltse and colleagues. The term isthmic spondylolysis is used to identify those patients who have sustained a lesion in the pars. Isthmic spondylolysis represents a pars lesion/defect that is believed to be a fatigue fracture of the bone. Most pars lesions identified in many studies occur at L5 (85%–95%). In a study of 4243 young athletes with low back pain, Rossi and Dragoni found that about one-half of those with spondylolysis also had concurrent spondylolisthesis. Significant progression of an associated spondylolisthesis is uncommon. There are data to support that there is not any increased risk of progression of spondylolisthesis with sports participation. When there is an increase in the anterior translation of 1 vertebral body on the other, it is usually correlated with an adolescent growth spurt, and typically without any symptoms. Therefore, once spondylolisthesis is identified in the adolescent athlete, the affected individual needs to be monitored radiographically through adolescence to assess for any progression of the spinal disease.
General population studies have shown pars lesions to be a common finding. In a prospective study of plain radiographs in 500 first-grade students, there was an overall prevalence of spondylolysis of 4.4% at age 6 years. All of these lesions identified in this study occurred without any symptoms. These diseases were then followed, and the number increased to 5.2% by age 12 years and 6% by adulthood. Comparatively, another cadaveric study reviewed plain radiographs of 4200 cadaveric spines and found an overall prevalence of 4.2%. However, the incidence of spondylolysis is different in adolescents who compete in athletics; large-scale studies of adolescent athletes reported rates of 8% to 14%.
There is definitively a significant variance of the incidence of spondylolysis in athletes who participate in certain sports. Some of the sports with the highest reported frequencies of pars lesions include gymnastics, weight lifting, throwing track and field sports, diving, wrestling, cricket, and crew. Sports that involve frequent flexion/extension motions of the lumbar spine, particularly when combined with rotation, may place athletes at more risk for pars fractures.
History and physical examination can be helpful in identifying a clinical pattern suggestive of the diagnosis of spondylolysis. However, by definition, additional spinal imaging is essential establish the diagnosis.
Athletes with spondylolysis typically present with insidious onset of extension-related low back pain. The athlete frequently also has an associated reduction in hamstring flexibility. Symptomatic spondylolysis typically presents with axial low back pain without radiation into the legs; however, the athlete may occasionally have radiating pain, numbness, or weakness if the disease affects the nerve roots. The pain typically occurs acutely after a specific traumatic event but may also occur after a relatively mundane event or may progress over time. The typical pain pattern associated with spondylolysis is usually worsened by activity and improved with rest. The athlete may complain of pain with impact, such as running or jumping. It is common for the symptoms to begin to develop toward the end of 1 sports season, subside after the season while the athlete is no longer stressing the area of disease, and then return once the athlete starts training for the next season. The distribution of pain varies depending on whether the lesion is unilateral or bilateral but can lateralize to the side of the unilateral lesion or be more generalized in the low back.
It is uncommon to have associated leg pain, paresthesias, or neurologic loss with isolated spondylosis. However, the presence of these symptoms does not eliminate spondylosis from the differential diagnosis. Rather, these findings should suggest the potential concomitant presence of spondylosis with spondylolisthesis or other diagnoses such as disk herniation in adolescent athletes. There are no pathognomonic findings on physical examination for spondylolysis; however, pain with extension and rotation may suggest disease of the posterior elements such as a pars lesion or facets. A special test to assess for potential spondylolysis is the 1-legged hyperextension maneuver. This maneuver is performed by having the patient stand on 1 leg and leaning backward. The maneuver has been proposed as a means of identifying the presence of a pars lesion, but a recent study of this test concluded that it had low sensitivity and specificity.
Several diagnostic imaging modalities are available for evaluating the pars in an athlete with suspected spondylolysis. However, there is significant controversy regarding the optimal imaging strategy, because of potential risks of radiation exposure in the growing adolescent spine. Given the relatively high prevalence of asymptomatic pars lesions in both the general population of adolescents and adolescent athletes, it is not enough just to visualize a pars lesion. Ideally, there is a clinical picture that is suggestive of disease of the pars, which is supported by the radiographic findings. Optimally, any radiographic pars defect needs to be identified as the source of pain and should be assessed for the potential of the lesion to heal. Therefore, in practical application, the clinician needs to assess the risks of radiation exposure from multiple imaging studies with the benefits of initial diagnosis and subsequent evaluation of pars defect healing.
Historically, plain radiography has been the primary imaging modality used in the identification, diagnosis, and observation of healing of pars lesions based on results of many published studies. The anteroposterior (AP) view may identify anatomic variants or developmental defects such as transitional vertebrae or spina bifida occulta, which is seen frequently in patients with spondylolysis. The lateral view may show spondylolisthesis or a lytic lesion. Typically, a spondylitic lesion seen in plain radiographs appears as a lucency in the area of the pars (see Fig. 1 ). Oblique views may show a stress reaction of the pars interarticularis and is identified as the pathognomonic neck of the Scotty dog lesion. However, the routine use of oblique views is discouraged in adolescent athletes, because of the increased dose of radiation and because only one-third of stress fractures can be identified on plain radiographs. Bone scan, single-photon emission computed tomography (SPECT), computed tomography (CT), and MRI have all been shown to be more sensitive than plain radiography in the identification of pars lesions.
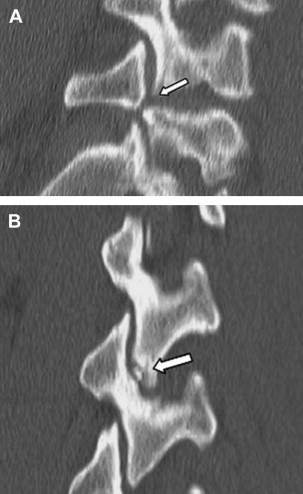
Plain radiographs should be followed by nuclear imaging with bone scan or SPECT. Radionuclide imaging, particularly SPECT, can be helpful in the diagnostic evaluation of adolescent athletes with low back pain. Bony lesions in which active bony turnover is occurring are indicated by increased uptake on the bone scan. Numerous studies have shown bone scan and SPECT to be more sensitive than plain radiography in the diagnosis of spondylolysis, and it seems to be superior to MRI and CT in this regard, as well. Multiple studies have also shown that a positive bone scan or SPECT scan correlates with a symptomatic pars lesion. This finding makes SPECT a particularly useful and sensitive screening tool in adolescent athletes with low back pain. However, significant limitation in the use of radionuclide imaging is low specificity, because there are several other abnormalities seen in the posterior elements of adolescents on SPECT or bone scan that do not represent pars lesions. Additional imaging, particularly with CT, is generally required to clarify the bony abnormality in a patient with a positive SPECT study ( Figs. 2 and 3 A ).