Fig. 4.1
The Kodama-Yamamoto TKA is shown
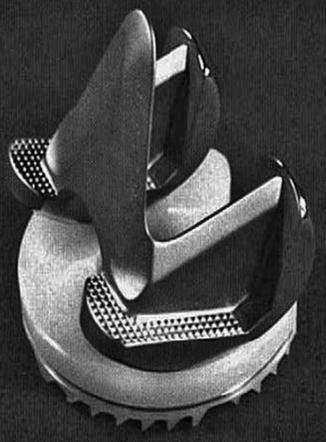
Fig. 4.2
The UCI TKA is shown
The Anatomical knee, designed by Townley, was the first TKA with a patellar button (Fig. 4.3). Femoral condyles and patellar flange were asymmetrical, while the largely nonconforming surfaces were designed in order to enhance movement and produce low constraint forces in an effort to decrease loosening [5]. This and the Leeds TKA were the first cemented cruciate retaining tricompartment Total Condylar TKAs. Townley tried to reproduce the normal anatomy of the knee so his design had different radii of curvatures in the frontal and sagittal planes. This design feature was expected to improve range of motion. Moreover, the retention of both cruciate ligaments was thought to promote stability and improve femoral roll back. Generally, Townley recognized and set many of the principles that are still used today in the field of TKA reconstruction. He strongly suggested the restoration of normal mechanical axis and alignment, emphasized proper implant sizing and the use of the thinnest possible polyethylene insert, supported the preservation of both cruciate ligaments to enhance stability and proprioception and noted the importance of patella resurfacing. The Anatomical knee is now distributed by Biopro as the Total Knee Original, however several other designs have been influenced by its principles including the AGC (Biomet), Axiom (Wright), Natural (Centerpulse), PCA and Duracon (Howmedica).
Fig. 4.3
The anatomical TKA is shown
The Leeds TKA was presented by Bahaa Seedhom at the same time as the Anatomic knee [6]. It had an anterior femoral flange with congruous patellar articulation throughout flexion and there was no need for patellar resurfacing. Femoral condyles were anatomical and asymmetrical and flared posteriorly in order to provide stability in the sagittal plane. Aiming to mimic the normal curvatures of the distal femur, bone surfaces were cut to create curved rather than flat surfaces. The tibial component was a single piece of polyethylene with two oval concaved discs and similar surface geometry to the femoral component allowing substantial anteroposterior and rotational laxity in flexion. An anterior bridge was formed to join the two parts of tibial insert having a recess in the middle to allow for preservation of the cruciate ligaments. There were right and left femoral and tibial components, a trend that would later be adopted by many future manufacturers (Fig. 4.4). Complexities in manufacturing techniques of the femoral and tibial implants and specific marketing reasons at that time made this knee design less popular among orthopaedic surgeons.

Fig. 4.4
The Leeds TKA is shown
The Ewald TKA consisted of an anatomical cobalt chrome femoral cap articulated with an all polyethylene tibial component (Fig. 4.5). The bearing surfaces were highly conformed in order to increase the contact area; however, the design was highly constrained and was not so popular.
Fig. 4.5
The Ewald TKA is shown
The designs introduced by the Hospital of Special Surgery (HSS) in New York proved to be very influential on the modern TKA. In 1971, Ranawat implanted the Duocondylar knee which was a symmetric, anatomical and cemented implant [7]. The linked femoral component had no anterior flange and both condyles were parallel. There were two separate tibial components providing minimal stability (Fig. 4.6). There was no provision for patellar replacement, but preservation of anterior and posterior cruciate ligaments was predicted. Although this was not a true condylar knee, significant conclusions were drawn from the experience of its use. Mainly, it was considered that resurfacing of the patellofemoral joint should be beneficial, preservation of both cruciate ligaments could probably interfere with the correction of deformities and fixation with cement might be insecure beneath the two separate tibial components. All these features would be taken into account and applied to the design of the next HSS implant, the Duopatella knee. Anatomical design and symmetry were preserved, but an anterior femoral flange was added in order to solve the problems of the Duocondylar knee. Moreover, a single tibial insert was used with a posterior cut out for preservation of the PCL. The anterior cruciate ligament was planned to be sacrificed. This implant was used in the treatment of patients with polyarticular rheumatoid arthritis with the expectation that the preservation of the PCL would enhance knee flexion. A few years later, the medial tip of the femoral trochlear flange was removed, creating right and left designs based on the asymmetry of the proximal femoral flange in order to reduce the medial overhang in small size knees. The Duopatella implant would evolve into the PFC Modular and PFC Sigma knee design (Depuy) as well as the Kinematic, Kinematic II, Kinemax and Kinemax Plus systems (Howmedica). At the beginning of 1979, Howmedica presented the PCA knee, which was anatomical with asymmetric medial and lateral femoral condyles similar to the Leeds and the original Townley implants. Its most important feature was the introduction of the porous coating concept. The femoral, tibial and patellar side were metal backed and sintered with 1.5 mm thick cobalt chrome beads.

Fig. 4.6
The duocondylar TKA is shown
The first representative of the functional approach concept was introduced during the mid 1960s, the Freeman – Swanson TKA [8]. In order to address the problem of high contact stresses, polyethylene wear and deformities, several suggestions were made. Both cruciate ligaments were resected in order to simplify the kinematics of the knee, reduce femoral rollback and permit a “roller-in-trough” design. Femoral cuts were made to be flat in order to preserve bone and no attempt was made to reproduce knee joint anatomy. A femoral component with a single radius of curvature was designed in order to articulate with a tibial implant of an identical radius, thus enlarging the contact areas considerably. The femoral component had a short stem, placed anteriorly, to fit into the hole left by the intramedullary guide used for alignment, while the tibial part had no stem but a dovetail to promote fixation with the bone (Fig. 4.7). There was only one implant size. Freeman’s contribution and innovative ideas were substantial. He emphasized the importance of creating and using specific instruments for proper implant alignment, introduced the use of spacers to check gaps remaining after the bone cuts and he recommended the use of tensor devices for ligament balancing. The first Freeman-Swanson design did not have a real anterior femoral flange and patella tracking was partly based on the femoral component and partly on the native joint. Later on, a long, flat patellar flange was added and the implant was renamed as the Imperial College London Hospital knee (ICLH) (Protek and Howmedica) and later as the Freeman-Samuelson knee.
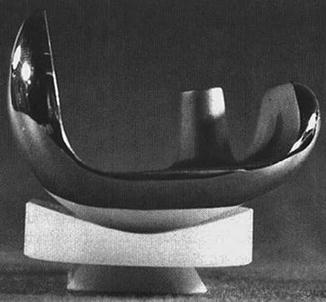
Fig. 4.7
The Freeman-Swanson TKA is shown
The first truly satisfactory, widely used and functional cruciate sacrificing implant was the Total Condylar TKA (TC) which was designed and introduced by Insall, Ranawat and Walker (Fig. 4.8). The TC combined the advantages of the anatomical bicondylar and the conforming surface design. The femoral component had a rounded medio-lateral geometry, while the sagittal radius mimicked the natural knee. There was an anterior femoral flange to improve patellar tracking and stability and a patellar button made of polyethylene was also provided. Bearing surfaces were of double dished shapes to provide better stability. The tibial component had a tibial peg to give additional but not primary fixation. Medio-lateral stability was enhanced by a central tibial eminence fitting a femoral intercondylar recess, while over-all knee stability was accomplished by combining joint surface geometry and soft tissue tension. The concept of flat bone cuts, creation of equal and parallel flexion and extension gaps and of careful ligament releasing was substantial. Keeping the principles of Total Condylar knee, Howmedica manufactured two cruciate retaining variants. These were the Cruciate Condylar knee, which preserved both cruciate ligaments, and the Posterior Cruciate Condylar knee, which preserved only the PCL. Some years later, Walker and Insall designed a central tibial post which engaged the femur in flexion in order to promote anteroposterior stability, ensure femoral roll back and avoid complications such as dislocations. This was the Total Condylar II design. The main problems of the Total Condylar knee were increased polyethylene wear, anterior instability and insufficient flexion. Burstein, following biomechanical studies, redesigned the implant shifting the point of contact of the joint more posteriorly and named it the Insall-Burstein Total Condylar knee. Adding a cam mechanism in order to reproduce the progressive rollback function of the PCL, posterior stabilized designs of the Hospital of Special Surgery were produced including the Insall-Burstein Modular posterior stabilized (IBPS II) (Zimmer), the Optetrak posterior stabilized (Exactech) and the Advance posterior stabilized (Wright Medical).
Fig. 4.8
The total condylar TKA is shown
Another significant and innovative design based on the functional approach was the mobile bearing knee (bicruciate retaining and rotating platform) introduced by Buechel and Pappas in 1977. The main concept was to achieve lower polyethylene contact stresses, while maintaining knee flexion and to avoid overload of the implant bone interfaces. The femoral component had a small posterior radius of curvature in order to provide normal kinematics during flexion and reduce the risk of polyethylene extrusion. This implant was named the New Jersey Knee System and would later evolve as the Low Contact Stress (LCS) and the LCS Rotating Patellar Replacement knee (DePuy) with the application of bone ingrowth surfaces into the components. Instead of having a dome shaped patella similar to the Total Condylar knee, the design of the patellar button was thick and anatomical in shape in order to properly fit into the femoral groove. In 1977, Polyzoides and Tsakonas presented another mobile meniscal bearing knee named the Gliding Meniscal knee (Zimmer). Similarly to LCS, articular surfaces in knee flexion were not fully congruent. This implant would later be improved and it evolved into a fully congruent rotational and gliding platform implant called the Rotaglide knee (Corin).
Related posts:
 The Long Term Outcome of Total Knee Arthroplasty. The Effect of Age and Diagnosis
A Brief History of Total Knee Arthroplasty
The Long Term Outcome of Total Knee Arthroplasty. The Effect of Age and Diagnosis
A Brief History of Total Knee Arthroplasty
 Long Term Survival of Total Knee Arthroplasty. Lessons Learned from the Clinical Outcome of Old Designs
Long Term Survival of Total Knee Arthroplasty. Lessons Learned from the Clinical Outcome of Old Designs
 Long Term Outcome of Total Knee Arthroplasty. The Effect of Implant Fixation (Cementless)
Long Term Outcome of Total Knee Arthroplasty. The Effect of Implant Fixation (Cementless)
 Long Term Outcome of Primary Total Knee Arthroplasty. The Effect of Body Weight and Level of Activity
Long Term Outcome of Primary Total Knee Arthroplasty. The Effect of Body Weight and Level of Activity
 Mid to Long Term Clinical Outcome of Medial Pivot Designs
Mid to Long Term Clinical Outcome of Medial Pivot Designs
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


