CHAPTER 21 Long-Term Patellofemoral Progression
 The natural history of the patellofemoral articulation after unicompartmental arthroplasty is poorly understood, and the majority of unicompartmental literature fails to adequately address and describe patellofemoral progression.
The natural history of the patellofemoral articulation after unicompartmental arthroplasty is poorly understood, and the majority of unicompartmental literature fails to adequately address and describe patellofemoral progression.



Introduction
Long-term survivorship of unicompartmental knee arthroplasty (UKA) is predicated on preoperative patient selection, obtaining proper limb alignment while avoiding overcorrection, and appropriate component position and sizing. An aspect of implant survivorship that is poorly understood is the natural history of arthritis progression in the adjacent tibiofemoral and/or patellofemoral compartments. However, one of the most common reasons cited for UKA failure is pain in one or more of the un-resurfaced compartments.1 The incidence and sequelae of patellofemoral compartment degeneration following UKA has been incompletely delineated. The purpose of this chapter is to summarize the natural history of patellofemoral compartment degeneration, and to describe the contribution of this degeneration to the long-term survival of UKA.
Preexisting Patellofemoral Arthrosis
The contribution of preexisting radiographic patellofemoral arthrosis and/or anterior knee pain to the survivorship of UKA has been described, yet remains a source of debate. Intuitively, preexisting patellofemoral arthritis and/or anterior knee pain should compromise the results of UKA, and many authors consider either of these findings to be contraindications to UKA.2,3 However, several studies have contradicted this assumption. In one short-term study, Beard et al.4 performed an intraoperative evaluation of the patellofemoral articulation in 824 medial UKAs using the Oxford (Biomet; Bridgend, United Kingdom) prosthesis. They noted full-thickness trochlear or patellar cartilage loss in 128 knees (13%). With minimum 1-year follow-up, the knees with cartilage loss did not have significantly worse Oxford scores or Knee Society scores, although patients with full-thickness patellar loss did have significantly worse Knee Society Functional Scores. Additionally, increasing severity of patellofemoral degeneration did not worsen the outcome. In another prospective study, Beard et al.5 evaluated the outcomes of 100 UKAs (Oxford, Biomet). Although 54% of knees had preoperative anterior knee pain and 54% had preoperative radiographic patellofemoral degeneration (including 10% with joint space obliteration), these knees had outcomes similar to the 46% without preoperative pain or degeneration. Knees with lateral patellofemoral degeneration faired slightly worse than knees with medial patellofemoral degeneration, but each of these groups still had good overall outcomes. The authors concluded that neither medial patellofemoral joint degeneration nor anterior knee pain should be considered a contraindication to Oxford UKA. Kuipers et al.6 also assessed the effect of preoperative patellofemoral joint involvement and reported on 437 Oxford UKAs evaluated at a mean of 2.6 years (range, 0.1–7.9 years). The authors found that preoperative patellofemoral osteoarthritis was not associated with decreased implant survival. In fact, they noted a paradoxical 70% reduction in revision risk for patients with preoperative patellofemoral osteoarthritis.
The longer term results of preexisting patellofemoral degeneration on the outcomes of UKA are less clear. There are several longer term outcome studies in which patellofemoral degeneration was not considered to be an absolute contraindication to UKA.7–15 Most of these failed to demonstrate significant differences in failure rates among those patients with and without preexisting patellofemoral arthrosis. However, Argenson et al.8 studied 160 UKAs (Miller-Galante; Zimmer, Warsaw, IN) for a mean of 5.5 years (range, 3–9.3 years) and found that two of their five revisions were secondary to patellofemoral arthritis. These authors noted that both of the revisions for patellofemoral arthritis also had preexisting patellofemoral degeneration. As a result of their findings, the authors now consider extensive loss of cartilage in the patellofemoral joint found on preoperative radiograph or intraoperative inspection to be a contraindication to UKA.
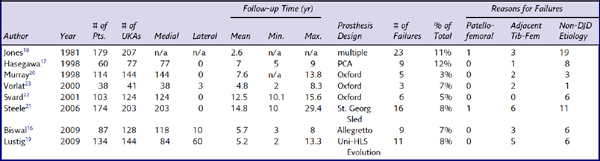
A substantial number of studies include patients with patellofemoral arthrosis as part of the inclusion criteria for UKA, but fail to mention the status of the patellofemoral joint clinically or radiographically at follow-up.16–23 These are shown in Table 21–1. Svard and Price,22 for example, reported the long-term results of 124 medial UKAs using the Oxford mobile-bearing prosthesis. In their cohort, “the state of the patellofemoral compartment was not used as a criterion for selection and no patient was rejected because of patellofemoral degeneration.” Six knees (4.8%) were revised for reasons unrelated to the patellofemoral compartment. However, there was no mention that the patellofemoral compartment was included as part of the follow-up evaluation. In the majority of these studies (see Table 21–1), there were no failures that were secondary to patellofemoral arthritis, and in two studies, only one failure was due to patellofemoral complications. It is therefore tempting to conclude that the inclusion of preoperative patellofemoral degeneration does not negatively affect outcomes. However, in each of these studies, there is no clear indication that the clinical or radiographic status of the patellofemoral joint was evaluated as one of the outcome measures. It may be that there truly were no complications attributable to the patellofemoral joint. Alternatively, it is possible that the authors were not looking for patellofemoral complications, given a bias that the patellofemoral joint is not a relevant source of pain in these patients. Therefore, we are guarded with respect to our interpretation of these reports and believe that meaningful conclusions regarding the extent to which preoperative patellofemoral involvement affects UKA longevity cannot be drawn based on these studies.
Long-Term Patellofemoral Arthritic Progression
We reviewed the literature for UKA outcome studies, with a specific emphasis on reports with long-term follow-up. Although there were several studies that specifically address patellofemoral complications following UKA, a surprising number of studies did not specifically include the status of the patellofemoral joint as part of their clinical and/or radiographic follow-up criteria.11,17,22–43 In these studies, it is difficult to conclude whether patellofemoral degeneration was simply not a source of clinical complication, or whether the patellofemoral joint actually impacted the results of UKA but was overlooked in the study design. As such, meaningful conclusions regarding the natural history of the patellofemoral articulation following UKA cannot be drawn from these studies.
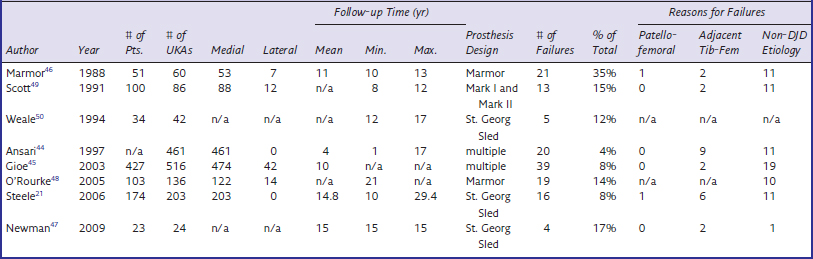
Table 21–2 lists another large subset of studies in which it is difficult to draw conclusions regarding the fate of the patellofemoral joint following UKA.21,44–50 In each of these outcome studies, the authors indicated that failures occurred secondary to “progression of disease” but, unfortunately, failed to differentiate if that progression occurred in the un-resurfaced tibiofemoral compartment or in the patellofemoral compartment (Fig. 21–1). Steele et al.21 reported on 203 medial UKAs (St. Georg Sled; Waldemar-Link, Hamburg, Germany) with a mean follow-up of 14.8 years (range, 10–29.4 years). The most common reason for failure in this cohort was “progression in another compartment.” Seven of 16 failures were secondary to progression. At least one revision was required because of progression of disease in both the lateral and patellofemoral compartments, but the authors did not specify the location of progression of the other six failures. O’Rourke et al.48 described the minimum 21-year results of 136 UKAs (Marmor; Richards Orthopaedics, Memphis, TN). In this series, the overall revision rate was 14.9% (19 knees) and the majority of revisions (9 knees) were secondary to “disease progression.” Again, the location of progression was not explicitly stated. The authors did, however, report that 75 knees (59%) had radiographic patellofemoral arthritis and 66 knees (52%) had contralateral tibiofemoral progression. Although progression occurred in both compartments, it is unclear if the progressions that lead to failure occurred in the tibiofemoral compartment, patellofemoral compartment, or both. Similarly, Gioe et al.45 reported on the 5- and 10-year survivorship of 516 UKAs (474 medial, 42 lateral) using prostheses from multiple manufacturers. A total of 39 failures were identified. The most common reason for revision was “progression of arthritis in the uninvolved compartments,” which accounted for 51.3% of the failures. Again, the location of the progression was not delineated. Thus, once again, the fate of the patellofemoral compartment is inconclusive based on these reports.
Table 21–2 Long-Term Studies Demonstrating Radiographic Evidence of Adjacent Compartment Degeneration, but without Delineation of Tibiofemoral or Patellofemoral Compartment Progression
< div class='tao-gold-member'>

Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


