Fig. 21.1
Painful patellofemoral joint in TKA. Radiological appearance at 5 years follow up

Fig. 21.2
Radiological appearance of a loose patella implant and patella fracture at 6 years follow up
In this review we present the effect of patella resurfacing or non-resurfacing on the long term outcome of TKA based on a critical evaluation of existing of quality studies.
History
It is important to focus on the history of resurfacing in order to reveal why controversies have arisen, and then focus on current knowledge related to this issue. It has been demonstrated, right from the beginning, that extensor mechanism dysfunction is the most common reason for revision after TKA [3, 4]. However, the first generation of TKAs did not routinely offer patellar surfacing. Isolated patellofemoral joint replacement has existed since the 1950s, when McKeever reported a series of 40 patients with patellar resurfacing using a Vitallium implant screwed into the patella [5]. In the 1970s, Blazina and Lubinus introduced femoral groove components combined with patella resurfacing [6, 7]. Initial results and complication rates were disappointing, leading to high TKA revision rates [8]. As time passed and first generation TKA survival rates improved, patellofemoral problems became more apparent [9]. The development of second generation TKA and the publication of satisfactory mid-term results regenerated scientific interest in the patellofemoral compartment of TKA. When retropatellar resurfacing became available, better outcomes in terms of improvement of function and pain relief were obtained.
Subsequently the following questions were raised: (a) Should the patella always be resurfaced? (b) What is the role of implant design? (c) Are the problems related to technical error during implant placement (wrong size, malalignment, femoral or tibial component malrotation etc.) preventable?
Anatomical Issues
According to Dennis [10], the load sustained by the patellofemoral joint varies from 0.5 to 1 times body weight during normal walking, 3–4 times body weight during stair climbing and 8 times body weight during knee flexion. This entire load is distributed on a narrow contact surface, the patellofemoral joint. When resurfacing the patella, the contact surface becomes even narrower leading to a load increase per area unit. Patella resurfacing decreases the contact surface more than non-resurfacing [11]. Singerman [12] demonstrated that patellofemoral contact forces are similar to normal without patella resurfacing in TKA, while Matsuda [13] declared that contact stress changes per area unit are affected by femoral component design, especially during knee flexion greater than 60°. It is important to note that some femoral component designs cause a patella inclination of more than 10° during knee flexion [14]. Evaluation of contact stress in metal backed patella implants with a mobile polyethylene insert showed both decreased and increased values [11, 15]. A literature search has shown that the developing contact stress per area unit is greater than the failure limit of the polyethylene insert [11]. It should be expected that higher wear rates and component failure would appear. Clinically, however, this did not happen often for several reasons (e.g., soft tissue adaptation, pseudomeniscus formation etc.). Recently, two important anatomical issues have appeared: anatomical alignment and the morphology of the distal femoral patella groove [16, 17].
Issues of Surgical Technique
Errors in surgical technique are the most common reason for patellofemoral joint complications. Thus surgery aims at correct alignment and balance of the extensor mechanism, and a surgeon must decide whether to replace the patellar or not [3, 18]. The surgical approach should be such as to avoid knee tightening and patella malalignment. Patellofemoral ligament resection is required [19]. Release of the patellofemoral ligament as described by Krackow [19] helps to laterally retract the patella which enhances exposure, thus improving patellar tracking and avoiding excessive soft tissue tightness. Principles of efficient patella resurfacing include (Fig. 21.3): (a) restoration of normal patellar thickness, which requires correct measurement, avoidance of over or under resection of the patella (a 1–2 mm decrease in patella thickness is perhaps allowed) (Fig. 21.4) [20]. (b) Creation of symmetrical patellar facets. Asymmetric inadvertent resurfacing occurs in 10–15 % of cases, even in the hands of experienced surgeons, which leads to increased patella inclination and instability [21]. (c) Preservation of intact patella vascularization by protecting the fat pad, the superior lateral artery of the knee during patellar release and intraosseous vascularization avoiding implants with one big central peg which may lead to patellar fracture (using implants with three pegs instead), (d) Patellar tracking restoration with lateral release or tibial tubercle displacement. Patellar tracking is better assessed when the tourniquet is released, before the soft tissues are sutured and by avoiding the stabilizing effect of the thumb when examining the knee during full range of movement, (e) Optimal femoral, tibial and patellar component orientation. Optimal femoral component placement is determined by 3° of external rotation, slight lateral displacement, neutral alignment in the sagittal plane and no anterior displacement [22]. Optimal tibial component placement is determined by slight lateral displacement in the frontal plane and rotationally centered in the medial aspect of the tibial tubercle. Finally, optimal patellar placement is determined by slight medial displacement of an implant of correct size and in neutral vertical alignment. Partial bursectomy using cautery, followed by some degree of denervation, is also recommended and (f) Avoiding Soft tissue impingement. Optimal patella implant design should meet the following criteria: (a) It should be symmetrical (oval central dome) or anatomical, (b) it should have three pegs instead of one big central one due to the risk of fracture and osteonecrosis, (c) it should not be metal-backed.
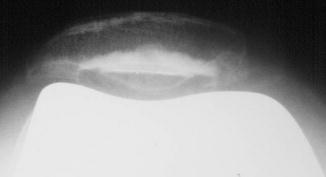
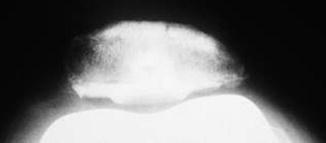
Fig. 21.3
Radiological appearance of satisfactory patella resurfacing at 12 years follow up
Fig. 21.4
Radiological appearance of a thick patella with overstuffing of the patellofemoral joint
When intraoperative evaluation reveals patellar malalignment (Fig. 21.5) and instability, malpositioning of the TKA implant should be excluded. If this is not the case, lateral patellar retinacular ligament release should be performed, to try to preserve the superior lateral geniculate artery and vastus lateralis tendon. If maltracking persists, medial imbrication should be performed [3]. Alternatively, tibial tuberosity transfer should be considered. It is a safe technique which requires the transferal of a large spiky bone fragment facing distally [23, 24].

Fig. 21.5
Radiological appearance of patella tilt and instability in bilateral TKA (right nonresurfaced and left resurfaced)
Surgical technique is probably more important than certain design features of the femoral and tibial components in minimizing the incidence of patellofemoral complications. A persistent problem with surgical technique is the variability of component alignment which is seen using the currently available alignment guides [4]. Eckhoff et al. [17] compared four different methods of determining tibial component rotation, for instance, and found a range of 20° from 2° internal rotation to 19° external rotation. A similar study has evaluated the alignment and rotation of the femoral component. Olcott and Scott [22] evaluated four commonly used methods of determining component rotation and found that flexion gap asymmetry occurred in 10–30 % of patients depending on the anatomical landmarks used to determine femoral component rotation [22].
Component Design
Early femoral component designs were not anatomical and were characterized by a shallow flat trochlear groove which resulted in a relatively high incidence of patellar subluxation and dislocation. The priority in early cruciate retaining components was minimal bone resection which resulted in the acceptance of a shallow groove [4]. Contemporary designs are anatomical and have incorporated a separate inter condylar bone cut in order to allow resection of adequate depth and replication of a normal anatomical trochlear groove [25]. Another design feature is the distal extent of the trochlear groove. Earlier designs did not provide support for the patellar component other than two small areas of point contact beyond 90° of flexion. By extending the metal surface of the trochlea farther distally, higher contact areas and lower contact stresses can be maintained beyond 90° of flexion [4]. This feature has been incorporated into some recent designs. There is evidence that this design feature is particularly advantageous when the patellar is left unresurfaced [13].
Replace or Not. The Decision (Figs. 21.6 and 21.7)

Fig. 21.6
Satisfactory radiological appearance of a resurfaced patella in an asymptomatic TKA at 16 years follow up

Fig. 21.7
Satisfactory radiological appearance of a nonresurfaced in an asymptomatic TKA at 14 years follow up
Some authors suggest routine resurfacing of the patella due to large numbers of cases with residual anterior knee pain, increased rates of both secondary patellar replacements (revision) and other reoperations in TKAs without patellar resurfacing [26–28]. Others find no reason to support routine patellar resurfacing [29–31]. They suggest that patella complications are found more often in a resurfaced group than in a group without resurfacing [29–31]. A selective decision based on factors such as patella thickness, the presence of preoperative anterior knee pain, the severity of degenerative changes in the patella or rheumatoid arthritis and the experience of the surgeon has also been suggested [32–34].
The native patella is more physiological and anatomical when compared with a resurfaced patella. Problems associated with patellar tilt and over stuffing of the patellofemoral joint are minimized when the native patella is not replaced. The most widely used argument against patellar resurfacing is the higher complication rate reported with patellar resurfacing. It is true that fractures, dislocations, extensor disruption and osteonecrosis have been reported without patellar resurfacing, but their incidence increases significantly and new complications appear with the increasing practice of patellar resurfacing [35–37]. New complications related to patellar resurfacing include component wear, dissociation, loosening, and patellar clunk syndrome [38, 39].
Arnold et al. [40] conclude that using a blood supply preserving approach and a biomechanically sound TKA without patellar replacement achieves excellent long term results. They also showed that the patellofemoral joint is an important problem after TKA [40]. Ogon et al. [31] have concluded that patellar complications were more often found in the resurfaced group than in the group without resurfacing. The results indicate no overall advantage of patella resurfacing compared with patella retention in the long run [41]. Barrack [41] has noted that every study to date supports the idea that kinematics are more abnormal when the patella is resurfaced than when it is retained. He also suggests that patello-femoral contact areas are higher and contact stresses are lower in the native patella compared with the resurfaced patella in TKA. Virtually every clinical study of bilateral knee arthroplasty in which one patella has been resurfaced and the other has not showed either equivalent results or a preference for the unresurfaced side. Laboratory and clinical data indicate that not resurfacing the patella is a viable if not a preferable option in most TKA patients [41]. Feller [42] reports that stair climbing ability was significantly better in the patellar retention group. Although there were no complications related to patellar resurfacing, in the mid-term no significant benefit was found from resurfacing the patella during TKA for osteoarthritis, unless it was severely deformed [42]. Proponents of patellar resurfacing argue that the native patella is more physiological and anatomical in the normal knee, but once the mechanics and surfaces of the joint are altered with arthroplasty, these advantages are lost. Patellar kinematics have been shown to be more variable after arthroplasty when compared with normal knees [43, 44]. With time, the prolonged effects of cartilage to metal contact become detrimental [36, 45]. High patellofemoral loads are also thought to contribute to cartilage deterioration over time [46]. This has been confirmed in vivo, based on numerous reports documenting significant cartilage erosion at the time of secondary resurfacing, despite the fact that healthy appearing cartilage was found at index TKA [47, 48]. In vitro and in vivo evidence of deterioration over time provides a compelling argument in favor of patellar resurfacing.
Revision rates due to patella resurfacing have been reported as high as 50 %, with an overall complication rate ranging from 5 % to 55 % in all TKAs [49, 50]. Poor results have been attributed to inferior prosthetic designs and surgical technique. Metal backed patella designs, which showed increased wear, loosening, and polyethylene dissociation, have provided the majority of undesirable data related to prosthetic design [51, 52]. This issue has improved with the use of all polyethylene, three pegged patella components [53]. Asymmetric patellar resection, patellofemoral joint overstuffing and excessive patella resection have also contributed to high complication rates. Surgical techniques for patella resection which emphasize patellar resection reproducing equal facet thickness, native patellar height and tracking and respecting vascular supply have produced complication rates from 0 % to 4 % [42, 54].
Various quality studies concerning patella resurfacing (including randomised controlled trials (RCTs), prospective studies, meta-analyses and systematic reviews) have been published but no final conclusion has yet been drawn. It has to be stressed that early studies were performed using non-anatomic and non-patella friendly femoral components which is, in our opinion, a serious negative confounding factor. Several investigators have reported superior results in patients having patellar resurfacing. Ranawat [55], in a 5–10 year follow up of 100 TKAs with patellar resurfacing, reports good to excellent results in the majority of patients with only a 2 % complication rate. Rand [56] evaluated 50 TKAs and showed an average Hospital for Special Surgery score of 92, 100 % good or excellent results, and no evidence of fracture, loosening, subluxation, or dislocation in mid-terms. Levitsky et al. [57] reports on 79 TKAs without resurfacing and on 13 bilateral TKAs with unilateral resurfacing. Of the 13 bilateral TKAs with unilateral resurfacing patient preference was 46 % equivocal, 46 % favoring resurfacing, and 7.7 % favoring non-resurfacing. Abraham et al. [58] evaluated 100 Variable Axis TKAs with 5–9 years follow up. Fifty three knees were non-resurfaced and 47 knees were resurfaced. No difference in pain or function was detected, but a statistically significant difference was observed in resting pain in the non-resurfaced knees. Overall, this study showed a trend to greater anterior knee pain in the non-resurfaced group. Picetti reports on 100 Total Condylar TKAs without patella resurfacing. An average follow up of 4.5 years 71 % good or excellent results were recorded. Forty percent of patients reported abnormal stair climbing and 29 % experienced patellofemoral pain. However, there was no control group and Total Condylar knee arthroplasty used had radically different design features than current designs. Boyd et al. [59] has shown that secondary resurfacing produced inferior results in their study of 891 Duopatellar TKAs at an average follow up of 6.5 years. Four hundred and ninety five patellae were not resurfaced and 396 were resurfaced. There was a 12 % complication rate in the non-resurfaced group compared to a 4 % complication rate in the primary resurfaced group. Ten percent of the patients who did not have resurfacing experienced postoperative patellofemoral pain compared to less than 1 % of the patients who had resurfacing. Most importantly, 10 % of patients who had secondary resurfacing for patellofemoral pain continued to have pain after secondary resurfacing and had a higher rate of skin slough, infection, and decreased ROM. However, this study included patients with inflammatory arthritis. When the analysis was restricted to patients with osteoarthritis, the complication rate was comparable between the two groups with 6 % of knees without resurfacing experiencing complications compared to 4 % among patients who had resurfacing. Again, this was an older design component that does not meet current design standards. Superior functional results have been reported with patella resurfacing. Schroeder-Boersch et al. [60] compared 20 resurfaced knees with 20 unresurfaced knees at a minimum of 2 years follow up. Better functional results were observed in the resurfaced knees, leading the authors to conclude that regular resurfacing is indicated in patients with OA. Twenty two patients with advanced patellofemoral disease who had bilateral TKAs were investigated by Enis et al. [61]. In all patients, the right side was treated with patellar resurfacing, whereas the left patella was not resurfaced. The resurfaced knees had superior isokinetic measurements, less patellofemoral pain, and were preferred by patients.
Results in the inflammatory arthropathy population have been consistently in favor of routine patellar resurfacing. Shoji [62] first reported on a population of 35 patients with RA who had bilateral TKAs with one side being resurfaced and the other side not. At an average follow up of 2.7 years, there was no difference in terms of pain, function, motion, or muscle power. Later, Kajino [63] evaluated the same group of patients 6 years after surgery. An increase in pain while standing, ascending or descending stairs, and patellofemoral tenderness in patients without patellar resurfacing was reported. Patients also presented radiographic erosive changes on the articular surface of the patella in previously unresurfaced patellas. Keblish et al. [34, 64] report no difference in clinical results between the two sides. Enis et al. [61] studied cases of bilateral TKA with and without patellar resurfacing using the Townley Knee (DePuy) and found that patients had a preference for the resurfaced side.
Barrack et al. [65] report the results of an RCT study using the Miller-Galante II total knee replacement which found no difference in knee score or patient satisfaction; however, 10 % of patients without resurfacing subsequently underwent resurfacing. Among the patients who had bilateral knee replacements with one side resurfaced and the other side not resurfaced, the knee scores were equivalent and patients expressed no preference for one side over the other. A minimum 5 year follow-up report of this same group of patients continued to show no significant difference between the groups [72]. The incidence of anterior knee pain increased in both groups, but more in the patients who had had resurfacing [53]. Bourne et al. [66] conducted a similar RCT study using the AMK TKA. Fifty patellas were resurfaced and 50 were not. At 2 years follow up less pain and greater flexion was recorded in patients without resurfacing. There were no differences reported in function, stair climbing, or extension torque. Four percent of the patients without resurfacing, however, required patellar resurfacing due to anterior knee pain. Later, Burnett and Bourne [47] report on these same 100 patients at 8–10 years follow up. At 4 years, pain was equal in the two groups and subjective pain questionnaires at final follow-up of 8–10 years showed that patients who had had resurfacing had less anterior knee pain with stair climbing and walking and overall higher patient satisfaction scores. A progression of cartilage degeneration during secondary resurfacing for pain was also observed.
Related posts:
 The Long Term Outcome of Total Knee Arthroplasty. The Effect of Age and Diagnosis
A Brief History of Total Knee Arthroplasty
The Long Term Outcome of Total Knee Arthroplasty. The Effect of Age and Diagnosis
A Brief History of Total Knee Arthroplasty
 Long Term Survival of Total Knee Arthroplasty. Lessons Learned from the Clinical Outcome of Old Designs
Long Term Survival of Total Knee Arthroplasty. Lessons Learned from the Clinical Outcome of Old Designs
 Long Term Outcome of Total Knee Arthroplasty. The Effect of Implant Fixation (Cementless)
Long Term Outcome of Total Knee Arthroplasty. The Effect of Implant Fixation (Cementless)
 Infected Total Knee Arthroplasty. Basic Science, Management and Outcome
Infected Total Knee Arthroplasty. Basic Science, Management and Outcome
 Long Term Outcome of Primary Total Knee Arthroplasty. The Effect of Body Weight and Level of Activity
Long Term Outcome of Primary Total Knee Arthroplasty. The Effect of Body Weight and Level of Activity
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


