Fig. 19.1
The Stanmore prosthesis (lateral view in flexion and extension) – a simple metallic hinge
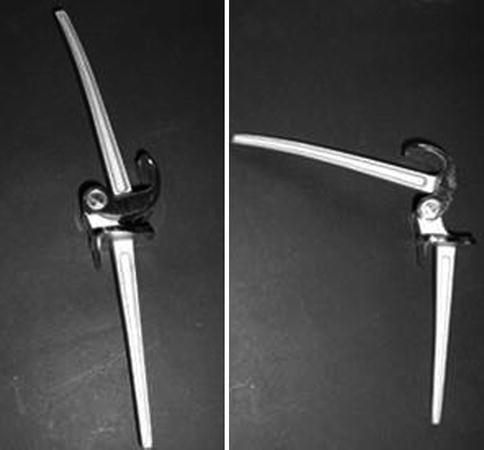
Fig. 19.2
The French GUEPAR prosthesis (lateral view in extension and flexion)
Fig. 19.3
St. Georg prosthesis (Waldemar Link GmbH, Hamburg, Germany). Anterior view. Classic hinge, precursor of the Endo-Modell prosthesis
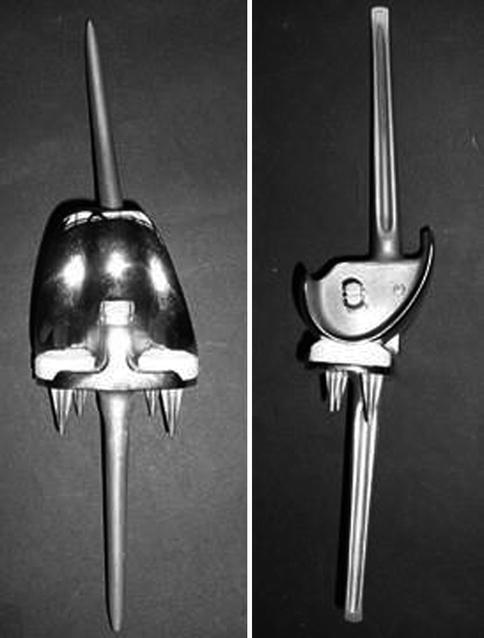
Fig. 19.4
Blauth Prosthesis (Aesculap, Tuttlingen, Germany), simple hinge with low friction design (femoral condyles on polyethylene)
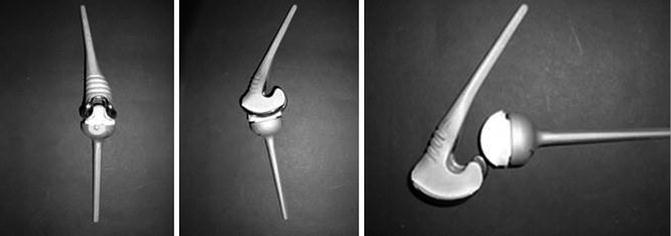
Fig. 19.5
Constrained condylar type design, the Sheehan prosthesis (1971). Anterior view, lateral view in slight flexion and demounted in lateral view. Low friction principle had been applied. Loosening, especially of the tibial component, was a constant concern
In early 1970s condylar TKA designs became increasingly popular due to their efficacy [14, 15]. Since then first generation of hinged prostheses became less attractive. In the late 1970s, the second generation hinged prostheses, the so called rotating hinge (RH) prostheses, were developed in order to facilitate reconstruction of certain more complex cases (difficult to address with condylar designs). Rotating hinges permitted motion both in the sagittal and the transverse plane (rotation), aiming at decreasing adverse high stresses on bone cement interface. Normal knee motion was better reproduced, since the so called home screw mechanism was feasible. Compared to first generation hinges, decreased loosening rates and improved gait pattern were achieved [2, 9, 16–18].
Condylar designs still remain the gold standard for a wide variety of cases, especially in primary TKA. However, certain indications are better met using constrained prostheses, and there is an ongoing controversy for the use of RHs or constrained condylar prostheses [19]. Defined indications and the choice of the appropriate type of RH TKA determines their outcome (in combination with other factors such as surgical technique, surgeon and patient related factors).
Types of Rotating Hinge Designs
Various designs of RH’s have been used so far. Their main difference is the design of the articulating mechanism. A widely used RH is the Endo-Modell (Waldemar Link GmbH, Hamburg, Germany). Having been used from the mid 1980s, numerous clinical studies showed satisfactory results (Fig. 19.6) [20–24]. The hinge consists of a T-shaped mechanism which articulates with the femoral condyles, allowing flexion and extension. The early design allowed distraction between the femoral bush and the tibial stud, but subsequently, in order to avoid dislocations, an antiluxation mechanism was routinely used. The distal part of the hinge ends as a femoral bush, of which the interior cavity is covered by a polyethylene layer. Inside this hollow bush or cylinder a metallic tibial stud is articulating, rising from the tibial component and allowing rotation (Fig. 19.6a). Rotation, although depending on degree of flexion, does not exceed 20–30°, since at this point the femoral condyles approach and decelerate against the intercondylar eminence of the tibial tray under the tension provided by the soft tissue envelope, which consists of the remaining capsule, ligaments, muscles and tendons. This implant was initially designed for primary arthroplasty preserving the patellofemoral joint (Fig. 19.6c), while subsequently it was also available with a patellar flange and button (Fig. 19.6a, b) in order to facilitate revision arthroplasty and to address patellofemoral osteoarthritis, with or without patellar resurfacing. According to the manufacturer, bone resections are minimal, especially with the initial design which had no femoral flange, resembling resections of condylar prostheses (Fig. 19.6c). Thus, despite its long cemented stems, revision is considerably facilitated.
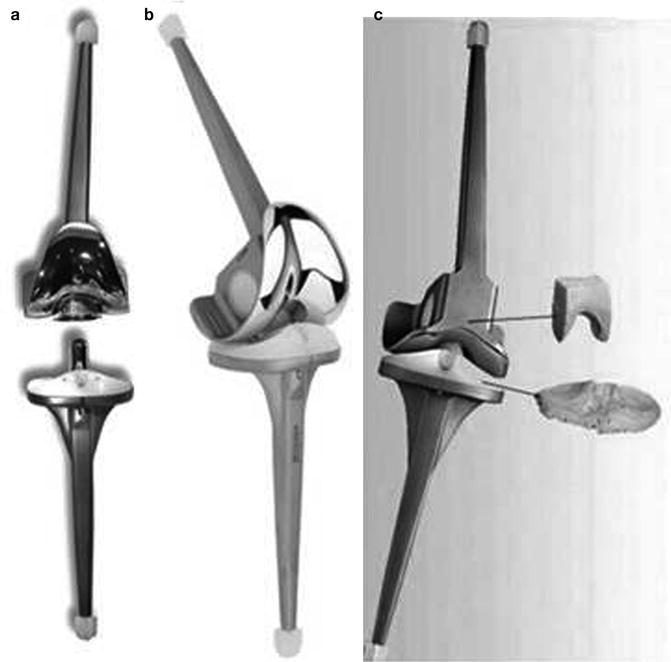
Fig. 19.6
The Endo-Modell prosthesis (Waldemar Link GmbH, Hamburg, Germany). The prosthesis disengaged (a), mounted in an oblique perspective (b) and almost from the front showing sparing bone resections (c). The former (c) is the initial design, preserving the patellofemoral articulation
Compared to the Endo-Model implant, two other RH’s, the Modular Segmental Kinematic Rotating Hinge (Howmedica, Rutherford, NJ) and the Noiles Prosthesis (Joint Medical Products, Stamford, CT) (Fig. 19.7) present a different design, since their axis is rotating inside the polyethylene tibial tray. Thus, rotation does not take place in the joint level but in a more wider and distal area, inside the tibial component. The Kinematic Rotating Hinge was designed exclusively for complex knee replacement, as after tumor resection or in complex knee revision with massive bone loss or ligamentous instability not amenable for a CCK arthroplasty [25, 26]. Initial designs had an all polyethylene tibial component while more recent designs have a metal-backed tibial component. Only minor differences, compared to the Kinematic Hinge, were present in the Noiles prosthesis although the latter demanded more extensive bone resections, especially in the tibia due to its larger tibial component (Fig. 19.7). Another hinge design, evolving out of the Noiles prosthesis and also exclusively used for revision, has been introduced in the S-ROM Modular Knee (Johnson & Johnson Orthopaedics, Raynham, MA) (Fig. 19.8). The hinge mechanism consists of a femoral peg fixed inside the tibial polyethylene stem which rotates inside the metallic tibial component. Rotation takes place beneath the polyethylene tray, reminding somewhat of a rotating platform knee. Since designed for revision purposes, it is equipped with adequately long femoral and tibial stems. Available for complex knee arthroplasty, and especially salvage surgery, is also the Finn knee rotating hinge, being the centerpiece of the OSS prosthesis (orthopaedic salvage system). This is a highly modular implant, providing a variety of components in order to address complex cases (Biomet, Warsaw, IN) (Fig. 19.9).


Fig. 19.7
Kinematic rotating and noiles hinge – classic rotating hinge designs with a femoral yoke mechanism and rotating tibial stem inside the tibial polyethylene
Fig. 19.8
S-ROM modular knee, consisting of a femoral hinge which is fixed inside the tibial tray which provides rotation within the tibial component, in a rotating platform manner
Fig. 19.9
The Finn rotating knee incorporated in one of the combinations of the OSS salvage systems. All these three prostheses are designated only for complex cases of knee arthroplasty
More recently (late 1990s), the Solution RT rotating hinge was introduced for primary and revision surgery (PLUS Endoprothetik AG, Switzerland, and since the year 2007 Smith & Nephew, Memphis, TN) in an attempt to reproduce normal kinematics, in terms of both home screw mechanism and femoral roll back (Fig. 19.10). If needed, femoral and tibial components are provided with modular stems, fixed with PMMA. The femoral rotation cone is articulated with the polyethylene liner inside a centrally placed bore permitting flexion, extension and rotation. Bone cuts are as sparing as with condylar prostheses except of the cuts for the femoral box. Although no specific patellar component is available, it is recommended, if needed, to use the patellar component of the respective condylar prosthesis. Recently, the same manufacturer (Smith & Nephew, Memphis, TN) introduced a similar RH implant, called Legion HK, aiming at the reproduction of normal knee kinematics (Fig. 19.11a). The same principles are present in the Zimmer NexGen Rotating Hinge prosthesis (Zimmer, Warsaw, IN). It seems that Solution RT, Legion HK and NexGen Rotating Hinge are rotating hinges of similar design and kinematics.


Fig. 19.10
The solution RT mounted and in components
Fig. 19.11
(a) Legion HK, modern rotating hinge prosthesis in flexion and slight rotation, (b) The rotating hinge mechanism of the Zimmer NexGen rotating hinge
Indications
There are various types of RH’s with different design and properties. When defining their indications one should interpret the literature based on different issues such as first generation implants, rotating or not rotating designs and on the fact that they are designated purely for revision or complex knee surgery. Skepticism regarding RH’s is justified, since major complications are more difficult to be successfully managed during revision, compared to condylar implants, usually due to severe bone loss. In primary TKA, the indications for RH based on the degree of bone deformity and ligamentous instability is not clearly defined. Similarly, it is difficult to define indications for either constrained condylar (CCK) or RH implants when revision or complex knee surgery has to be performed. Several authors [2, 9, 27–29] use RH arthroplasties in revision and complex knee surgery only and propose strict indications such as (a) anteroposterior instability, especially if there is a very large flexion gap compared to the extension gap, (b) complete absence of the medial collateral ligament, (c) lateral rotational instability due to complete absence of any lateral stabilizing structures and (d) complete absence of any functional extensor mechanism resulting in a swing-through gait [27].
In North America, hinged implants were almost completely abandoned until the appearance of the RH’s. In Central Europe, instead, hinged implants and especially RH’s were extensively used, resulting in a respectable experience, even in primary RH arthroplasty. The indications for example for the primary Endo-Model TKA, as published by its developers, included gross deformity and instability, since deformity correction and balancing are easily achieved, while with condylar implants similar results can be achieved only by applying strict indications and performance of meticulous and precise surgical techniques [1]. Another indication for primary RH TKA is rheumatoid arthritis, since it can lead to progressive capsuloligamentous deficiency [1]. Condylar TKAs, in rheumatoid knees may develop late (after the 5th postoperative year) recurrence of malalignement without component loosening.
Clinical Outcome of RH’s
When evaluating RH’s, it is necessary to separate primary arthroplasty from complex knee surgery, either revision or salvage surgery. Moreover, RH implants proved more satisfactory than first generation hinged implants since complications, especially infection and loosening, were significantly reduced and walking pattern was improved [2, 9, 16–18, 30]. Therefore it seems inappropriate to restrict the use of RH TKA based on the memory of the poor results of fixed hinged implants. On the other hand, fixed hinge designs have been improved in the recent years. For example, Blauth TKA (Aesculap, Tuttlingen, Germany), a fixed hinge following the low friction principle, showed a 98 % survival rate at 10 years and 94 % at 20 years, though in low demand and senile patients [31]. Such high survival rates were also recorded in another study with the same implant. However, function seemed compromised, since average flexion was 95° only and half of the patients were able to stand up from a seated position with the support of their arms only, indicating limited knee flexion [32].
A literature search for RHs efficacy and clinical outcomes in cases with revision and complex knee surgery, no high quality studies (RCTs) were found. Most of them are relatively small cohort studies, retrospective and with a short follow-up. Therefore, no evidence based conclusions can be drawn.
The Noiles prosthesis, one of the early types of RH’s (Fig. 19.8a), was evaluated in a small series of 18 complex TKAs. A 56 % failure rate was reported in terms of a HSS-score less than 60 points at 5 years follow up [2]. Major complications included femoral component subsidence, 5.1 mm on average, more pronounced in rheumatic patients (10 mm on average). Although such results seem disappointing, these cases were demanding salvage procedures. The Kinematic Rotating Hinge (Fig. 19.8a) was evaluated in a series of 38 knees (15 primaries and 23 revisions) available for follow up, out of 50 complex TKAs, with strict patients’ selection criteria [9]. Clinical outcome in terms of pain, function and ROM was found improved at an average of 50 months follow up. A high complication rate was recorded including patellofemoral problems in 13 knees (34 %), deep infection in 8 knees (21 %), mechanical failure of the components in 8 knees (21 %) and loosening in 3 (7.9 %). Such high complication rates in mid term are not acceptable, but one has to keep in mind the severity of the cases. The authors stated that RH’s should be reserved only for knees with complete absence of medial or lateral capsuloligamentous structures.
In contrast, satisfactory clinical outcomes have been reported with other RH’s designs implanted as primary TKA with appropriate indications. Such an example is the Endo-Modell RH implant. In an initial retrospective report of 1,837 primary RHs (1,639 knees were available for follow up), a low aseptic loosening rate of 0.8 % and an infection rate of 1.9 % was documented at an average follow-up of 6.5 years [20]. In 1.8 % of the cases postoperative patellectomy or hemipatellectomy, due to severe patellofemoral pain, was performed, while mild patellofemoral pain was recorded in 12.6 % of them. Material failure, dislocations and instability occurred in 2 % of cases. Fifty-four per cent of the patients were pain free and 40 % reported mild pain only. Overall rate of patient satisfaction was 95 %, with 83 % of the patients reporting to be very satisfied and 12 % satisfied. Survival rate, with revision for any reason as the end point, was 94 % at 8 years follow up. In a similar retrospective, 7–8 years follow up study, of 230 primary TKAs using this implant, mainly for severe valgus or varus deformity, for rheumatoid arthritis and posttraumatic arthritis, complication rates were low (2.6 % for aseptic loosening, 0.4 % for malalignement, 2.6 % for infection, 0.4 % for nervous lesions and 1.7 % for patellofemoral complaints addressed by patellectomy) [21]. Authors showed these complication rates were found lower when compared to those recorded with the use of the fixed St. Georg hinge (with a follow up existing 20 years). It would be interesting to focus on the overall postoperative patellofemoral pain rate. Engelbrecht, one of the developers of this RH implant, suggested that when the femoral component is placed in extension, condyles shift anteriorly increasing the forces in the patellofemoral joint and thus triggering equivalent symptoms [1]. Apart of surgeon related factors leading to patellofemoral symptoms, other implant related issues such as the trochlea design remain a matter of concern in hinged implants since the articulating mechanism restricts the depth of the trochlea. Infection rate is also high when compared to condylar implants mainly due to the bulky structure of the implant and the complexity of the surgery [31, 33]. In another study with 100 Endo-Modell primary TKAs, a 94 % survival rate at a mean follow up of 11 years was recorded leading to the conclusion that results were favorably comparable to condylar implants [24]. Early infection rate was 2 %, while patellofemoral maltracking was observed in 6 % of the procedures. Neither progressive radiolucent lines and migration, nor polyethylene wear were found. However, in another long term study with 98 primary RH TKAs the cumulative survival rate was 79.8 % at 10 years and 75.8 % at 15 years [34]. The authors suggested the use of RH arthroplasty in instability and revision cases only.
Related posts:
 The Long Term Outcome of Total Knee Arthroplasty. The Effect of Age and Diagnosis
A Brief History of Total Knee Arthroplasty
The Long Term Outcome of Total Knee Arthroplasty. The Effect of Age and Diagnosis
A Brief History of Total Knee Arthroplasty
 Long Term Survival of Total Knee Arthroplasty. Lessons Learned from the Clinical Outcome of Old Designs
Long Term Survival of Total Knee Arthroplasty. Lessons Learned from the Clinical Outcome of Old Designs
 Long Term Outcome of Total Knee Arthroplasty. The Effect of Implant Fixation (Cementless)
Long Term Outcome of Total Knee Arthroplasty. The Effect of Implant Fixation (Cementless)
 Infected Total Knee Arthroplasty. Basic Science, Management and Outcome
Infected Total Knee Arthroplasty. Basic Science, Management and Outcome
 Long Term Outcome of Primary Total Knee Arthroplasty. The Effect of Body Weight and Level of Activity
Long Term Outcome of Primary Total Knee Arthroplasty. The Effect of Body Weight and Level of Activity
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


