Chapter 45 Light Agents
OVERVIEW.
Laser stands for light amplification by stimulated emission of radiation. Cold (low power) lasers use less than 60 mW of power and produce little or no thermal response. The He-Ne cold laser has generated interest in physical therapy because of its purported wound healing and analgesic effects (when used over acupuncture or trigger points).1–5 Users must obtain an investigational device exemption from the FDA for this class III medical device. In 2002, the FDA approved its use for carpal tunnel syndrome.5,6
SUMMARY: CONTRAINDICATIONS AND PRECAUTIONS.
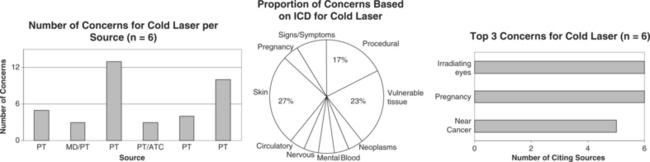
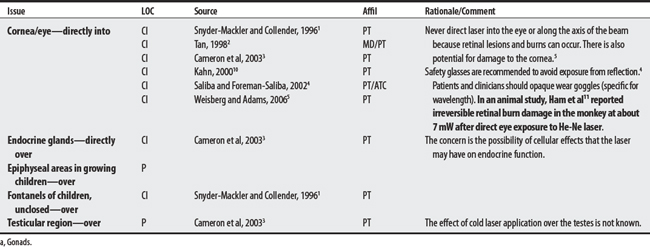
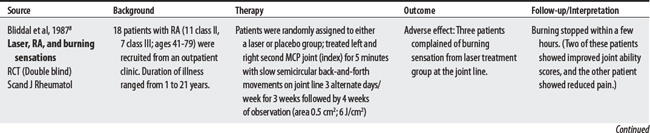
Six sources cited a total of 23 concerns for cold laser. Concerns ranged from 3 to 13 per source, with a physical therapist citing the largest number. The largest proportion of concerns were listed under skin, vulnerable tissue, or procedural categories. Many concerns are inadequately explained for cold laser; perhaps the basis for some concerns is a lack of information on its effects on tissue.3 The most frequently cited concern was irradiating the eyes (a concern well supported by evidence), use during pregnancy, and application near cancerous lesions.
CONTRAINDICATIONS AND PRECAUTIONS

D50-D89 DISEASES OF 3BLOOD AND BLOOD-FORMING ORGANS

F00-F99 MENTAL AND BEHAVIORAL DISORDERS

G00-G99 DISEASES OF THE NERVOUS SYSTEM

I00-I99 DISEASES OF THE CIRCULATORY SYSTEM

L00-L99 DISEASES OF THE SKIN AND SUBCUTANEOUS TISSUE

O00-O99 PREGNANCY, CHILDBIRTH, AND PUERPERIUM

R00-R99 SYMPTOMS, SIGNS, AND ABNORMAL CLINICAL AND LABORATORY FINDINGS (NOT ELSEWHERE CLASSIFIED)


1 Snyder-Mackler L, Collender SL. Therapeutic uses of light in rehabilitation. In Michlovitz SL, editor: Thermal agents in rehabilitation, ed 3, Philadelphia: F.A. Davis, 1996.
2 Tan JC. Practical manual of physical medicine and rehabilitation: diagnostics, therapeutics, and basic problems. St. Louis: Mosby, 1998.
3 Cameron MH, Perez D, Otaño-Lata S. Electromagnetic radiation. In: Cameron MH, editor. Physical agents in rehabilitation: from research to practice. St. Louis: Saunders, 2003.
4 Saliba E, Foreman-Saliba S. Low-power lasers. In Prentice WE, editor: Therapeutic modalities for physical therapists, ed 2, New York: McGraw-Hill, 2002.
5 Weisberg J, Adams D. Low-level laser therapy. In: Hecox B, Mehreteab TA, Weisberg J, editors. Integrating physical agents in rehabilitation. Upper Saddle River (NJ): Pearson Prentice Hall, 2006.
6 Basford JR. Therapeutic physical agents. Delisa JA, editor. Physical medicine and rehabilitation: principles and practices, ed 4, vol 1. Philadelphia: Lippincott Williams & Wilkins, 2005.
7 Gabel P. Does laser enhance bruising in acute sporting injuries? Aust J Physiother. 1995;41:273-275.
8 Bliddal H, Hellesen C, Ditleven P, et al. Soft-laser therapy of rheumatoid arthritis. Scand J Rheumatol. 1987;16:225-228.
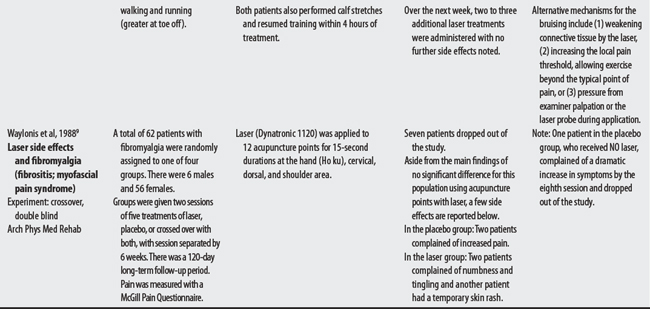
9 Waylonis GW, Wilke S, O’Toole D, et al. Chronic myofascial pain management by low-output helium-neon laser therapy. Arch Phys Med Rehab. 1988;69(12):1017-1020.
10 Kahn J. Principles and practice of electrotherapy, ed 4. New York: Churchill Livingstone, 2000.
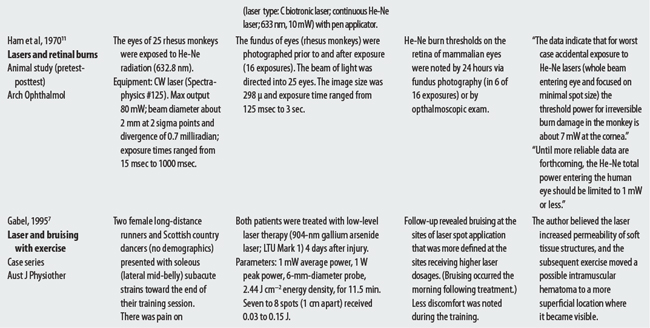
11 Ham WTJr, Geeraets WJ, Mueller HA, et al. Retinal burn thresholds for the helium-neon laser in the rhesus monkey. Arch Ophthalmol. 1970;84(6):797-809.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


