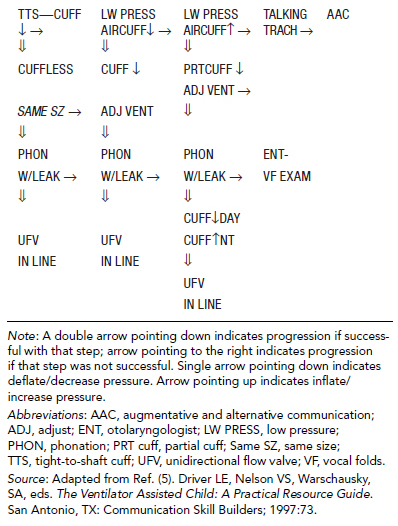
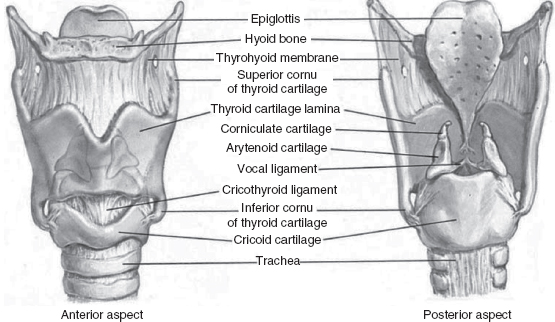
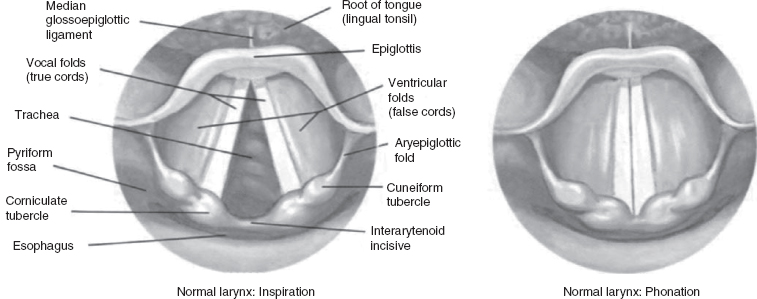
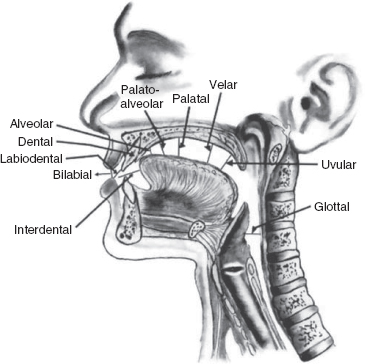
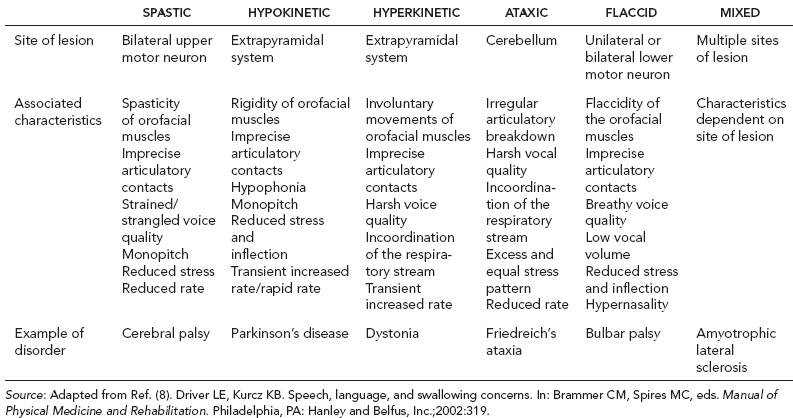
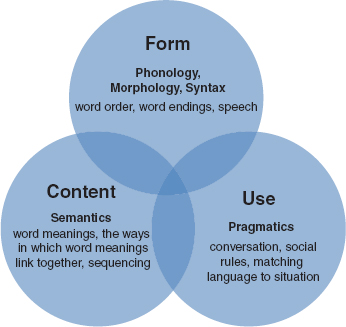
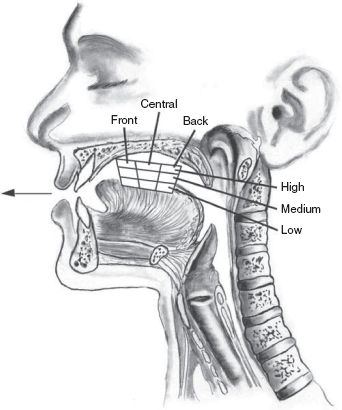
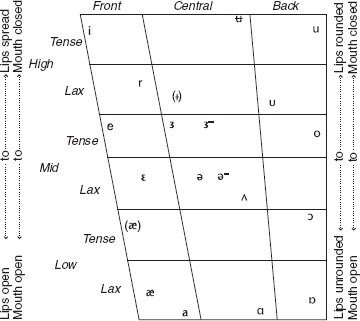
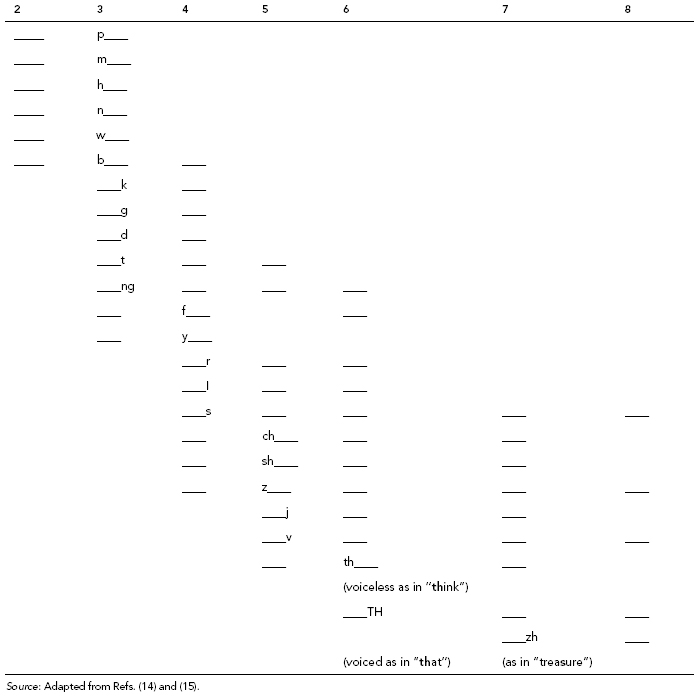
4 LANGUAGE DEVELOPMENT AND DISORDERS OF COMMUNICATION AND ORAL MOTOR FUNCTION Lynn Driver, Rita Ayyangar, and Marie Van Tubbergen Communication, as defined by the National Joint Committee for the Communicative Needs of Persons with Severe Disabilities (1), refers to “any act by which one person gives to or receives from another person information about that person’s needs, desires, perceptions, knowledge, or affective states. Communication may be intentional or unintentional, may involve conventional or unconventional signals, may take linguistic or non-linguistic forms, and may occur through spoken or other modes.” Communication is clearly a dynamic process used to exchange ideas, relate experiences, and share desires. Communication takes a variety of forms, including speaking, writing, gesturing, and sign language. As we know, interference with the physical ability to perform any of these acts has a significant impact on communication. Oral motor and neurologic impairments that affect communication may also significantly affect swallowing. The purpose of this chapter is to provide a basic understanding of the acts of communication and swallowing, as well as an understanding of the primary disorders resulting from abnormal development or acquired injury of structures or systems related to these acts. The chapter is divided into two sections. The first section describes speech and language development and disorders through the exploration of four main topics: • The primary anatomic systems of speech along with brief examples of deficits that result from disruption in these systems • The primary components of speech and language, including milestones for acquisition • Common speech and language disorders, both developmental and acquired, as well as common associated disorders • A brief description of speech and language assessment and intervention The second section describes feeding and swallowing processes and disorders and includes the following: • Development of feeding skills, including expected milestones • Anatomy and physiology of the swallowing mechanism • Common disorders of deglutition, both congenital and acquired • Feeding and swallowing assessment and intervention SPEECH AND LANGUAGE DEVELOPMENT AND DISORDERS Within the field of communication sciences and disorders, we think of communication as broadly comprising speech and language. Speech generally refers to aspects of communication that involve motor output for production of speech sounds. Production of speech sounds requires functional input from respiratory, phonatory, and articulatory systems (Table 4.1). Language generally refers to the process by which we both encode and process meaning within messages, and is divided into three primary components: form, content, and use. These components can be further subdivided based on five key aspects of language—specifically, phonology, morphology, syntax, semantics, and pragmatics. ANATOMY OF SPEECH SYSTEMS As noted previously, production of speech requires input from respiratory, phonatory, and articulatory systems. An airstream is generated by the lungs, passes through the vocal cords, and is then shaped by the articulators to form speech sounds. Impairments in any of these systems most likely will have a significant impact on speech production. TABLE 4.1 COMPONENTS OF SPEECH RESPIRATORY PHONATORY ARTICULATORY Upper Airway Larynx Lips Nose Vocal Cords Tongue Mouth Cartilage Palate Pharynx Muscle Nasopharynx Mucous Oropharynx Membrane Hypopharynx Ligaments Lower Airway Trachea Lungs Respiration The respiratory system is composed of the upper and the lower airways. The upper airway consists of the nose, mouth, pharynx, and larynx, and the lower airway consists of the tracheobronchial tree and the lungs (2). UPPER AIRWAY. The upper airway has many functions. The mucous membranes covering much of the upper airway structures are softer, looser, and more fragile in infants and young children than in older children and adults, and more susceptible to edema and injury from trauma. NOSE. All children are obligate nasal breathers during the first 6 months of life, during which time the soft palate is in close anatomic approximation with the epiglottis. This factor, combined with the relatively large size of the tongue relative to the oral cavity at this age, renders nasal patency essential for maintaining an airway. Those children with nasal obstructions from conditions such as choanal atresia are at risk for respiratory compromise (cyanosis) during feeding. MOUTH. The lips, mandible, maxilla, cheeks, teeth, tongue, and palate are the most important components of the oral cavity with regard to manipulation of airflow for respiration and speech production. The infant tongue takes up a larger area in the mouth and rests more anteriorly in the oral cavity than that of the adult. There are numerous congenital craniofacial anomalies, often associated with syndromes, that have an adverse impact on airflow. Some anomalies, such as cleft palate, prevent sufficient valving of the airstream, resulting in inaccurate production of speech sounds. Other anomalies, such as glossoptosis (oropharyngeal or hypopharyngeal obstruction during feeding caused by tongue retraction; common in disorders such as Pierre Robin sequence), can result in blockage of the airstream and subsequent respiratory distress. PHARYNX. The pharynx, a muscular tube shared by the respiratory and digestive tracts, is sometimes referred to as the aerodigestive tract, and serves vital functions for both respiration and swallowing. It is divided into three portions: the nasopharynx, oropharynx, and the hypopharynx. The pharynx in an infant is gently curved, and as the child grows and develops, the angle increases to approximately 90 degrees. The nasopharynx is the portion of the pharynx directly behind the nasal cavity, extending from the roof of the nasal cavity to the roof of the mouth. In addition to conducting air, the nasopharynx acts as a resonator for voice. The eustachian tubes from the middle ear open into the nasopharynx. The oropharynx is that portion of the pharynx directly behind the oral cavity, extending from the roof of the mouth (pharyngeal aspect of the soft palate) down to the base of the tongue, at the level of the tip of the epiglottis. Movement of the pharyngeal walls in this portion, together with elevation of the soft palate and the posterior portion of the tongue, is crucial for velopharyngeal closure. Inadequate closure, or velopharyngeal incompetence, can result in disordered speech production. The hypopharynx extends from the base of the tongue at the level of the hyoid bone and tip of epiglottis down to the entrance of the larynx and esophagus. Lower Airway The lower airway consists of the tracheobronchial tree and the lungs. The tracheobronchial tree consists of a system of connecting tubes that conduct airflow in and out of the lungs and allow for gas exchange. TRACHEA. The trachea is situated anterior to the esophagus, beginning at the cricoid cartilage and extending inferiorly to the carina, where it bifurcates into the right and left main-stem bronchi. It is composed of C-shaped cartilage rings joined by connective tissue. These cartilage rings assist in keeping the trachea open during breathing. As noted previously, the mucous membranes of the trachea are softer, looser, and more fragile than those of the adult and more susceptible to damage, increasing the risk of obstruction from edema or inflammation. LUNGS. The lungs are situated in the thoracic cavity, enclosed by the rib cage and diaphragm, the major muscle of ventilation, which separates the thoracic cavity from the abdominal cavity. The diaphragm in an infant is flatter than that of an adult, resulting in less efficient functioning for respiration. The air passages in infants and small children are much smaller, increasing their susceptibility to obstruction. The respiratory bronchioles, alveolar ducts, and alveoli grow in number until about 8 years of age, after which they continue to grow in size. Impairments in lung function can occur as a result of birth-related conditions such as bronchopulmonary dysplasia (BPD) and diaphragmatic hernia, or due to acquired disorders such as spinal cord injury (SCI). These impairments often require tracheostomy and/or mechanical ventilation, which in turn have an impact on speech production. CONTRIBUTION OF RESPIRATORY DYSFUNCTION TO SPEECH DISORDERS Speech disorders related to respiratory dysfunction are often secondary to the presence of tracheostomy and/or ventilator dependence. The primary diagnoses of children requiring chronic tracheostomy and/or ventilator dependence include conditions due to trauma such as brain injury, SCI, and direct injury to the trachea; congenital conditions; progressive neurologic disorders; and acquired nontraumatic conditions such as Guillain–Barré syndrome and anoxic encephalopathy (3). It is important to note that the causes of respiratory failure and subsequent need for mechanical ventilation are not always respiratory disease or disorder. The lungs themselves may be healthy, but access to them or the systems that contribute to their function may be impaired. A primary means of airway management in the presence of chronic respiratory insufficiency is a tracheostomy. A tracheostomy is an artificial opening created between the outer surface of the neck and the trachea between the second and third tracheal rings. The opening itself is referred to as the stoma, and the tracheostomy tube inserted into the trachea through the stoma serves to maintain the opening, as well as provide means for connecting mechanical ventilatory devices. Tracheostomy provides a secure airway, long-term airway access, and a means for interface with mechanical ventilatory devices, and as such, is the most frequently used method of airway management. Placement of the tracheostomy tube diverts airflow away from the trachea through the tube and out the neck, bypassing the upper airway, including the vocal cords. Depending on the size and type of tracheostomy tube, a portion of the airflow will still pass around the tube and through the vocal cords; this may or may not be sufficient to produce sound. In the event that it is not sufficient, options to facilitate sound include downsizing of the tracheostomy tube to a smaller diameter and use of a unidirectional flow valve such as the Passy–Muir valve (4), which directs greater airflow through the upper airway and out the nose and mouth. Table 4.2 shows a decision flow chart for manipulating factors related to the tracheostomy tube in order to facilitate voicing. TABLE 4.2 TRACHEOSTOMY TUBE DECISION FLOW CHART Phonation The phonatory system comprises the larynx, and provides the sound source for speech. When this sound source is disrupted, it may result in alterations in voice quality, thus affecting communication. The larynx is made up of cartilage, ligaments, muscles, and the mucous membrane. It protects the entrance to the lower airway and houses the vocal cords (Figure 4.1) (6). Sound is generated in the larynx, and that is where pitch and volume are manipulated. The strength of expiration of air from the lungs also contributes to loudness, and is necessary for the vocal folds to produce speech (Figure 4.2) (6). Most of the muscles of the larynx receive their innervation via the recurrent laryngeal branch of the vagus nerve. This branch descends downward and wraps around the aorta, and for this reason, children who undergo cardiac surgery can sometimes experience voice disorders. If the recurrent laryngeal nerve is stretched or damaged during surgery, innervation to the vocal cords can be disrupted, and vocal hoarseness can occur. FIGURE 4.1 The larynx. CONTRIBUTION OF PHONATORY DYSFUNCTION TO SPEECH DISORDERS Speech disorders related to phonatory dysfunction are generally classified as voice disorders, and include dysphonia (abnormal voice quality) and aphonia (loss of voice). Dysphonia is an impairment of voice secondary to cranial nerve involvement, laryngeal pathology, or tracheostomy, and is characterized by varying degrees of breathiness, harshness, and vocal strain. Dysphonia may be a prominent feature of dysarthria related to cranial nerve involvement. Laryngeal pathologies resulting in dysphonia may include polyps, granulomas, nodules, or other lesions affecting the vocal fold mucosa. A common vocal fold trauma resulting in dysphonia is traumatic intubation following serious injury requiring assisted ventilation. Articulation/Resonance The articulatory/resonatory system is composed of the structures of the oral and nasal cavities, which modulate the airstream into the acoustic waveforms perceived as speech. Articulators responsible for production of speech sounds include the lips, tongue, and palate. FIGURE 4.2 The vocal cords. FIGURE 4.3 Places of articulation. In addition to the placement of articulators, successful production of accurate speech sounds requires adequate functioning of the oral and nasal cavities as resonating chambers (resonance). Modulation of the airstream by these structures is a complex process that relies on intact structures as well as precise neuromuscular coordination. Figure 4.3 illustrates where various articulators are located, as well as places of articulation for various speech sounds. Impairment in one or more of these components is likely to result in a disorder of articulation/resonance. CONTRIBUTION OF ARTICULATORY/RESONATORY DYSFUNCTION TO SPEECH DISORDERS Speech disorders related to articulatory/resonatory dysfunction include disorders that result from impairment in any component of the articulatory/resonatory system, and as such are quite comprehensive. They include all motor speech disorders, including dysarthria and apraxia, as well as disorders resulting from congenital conditions such as cleft palate. Although the three components of speech described previously are considered separately as individual components, they function as a single coordinated and interactive unit for production of speech, and as such, are subsystems of a complex motor act requiring precise coordination of muscle groups. It is easy to understand how impairments in any of these components can have an impact on communication, as the extent and complexity of the speech system make it susceptible to the influence of a myriad of factors. Motor speech disorders are a collection of communication disorders involving retrieval and activation of motor plans for speech, or the execution of movements for speech production (7). Subcategories include dysarthria and apraxia of speech. Motor speech disorders occur in both children and adults and may be acquired or developmental in nature (Table 4.3). Dysarthria refers to a group of related motor speech disorders resulting from impaired muscular control of the speech mechanism, and manifested as disrupted or distorted oral communication due to paralysis, weakness, abnormal tone, or incoordination of the muscles used in speech (Table 4.4) (8). It affects the following: • Respiration: respiratory support for speech, breathing/speaking synchrony, sustained phonation • Phonation/Voice: loudness, quality • Articulation: precision of consonants and vowels • Resonance: degree of airflow through nasal cavity • Prosody: melody of speech, use of stress and inflection Movements may be impaired in force, timing, endurance, direction, and range of motion. Sites of lesion include bilateral cortices, cranial nerves, spinal nerves, basal ganglia, and cerebellum. Associated characteristics of dysarthria include slurred speech; imprecise articulatory contacts; weak respiratory support and low volume; incoordination of the respiratory stream; hypernasality; harsh or strained/strangled vocal quality; weak, hypophonic, breathy vocal quality; involuntary movements of the oral facial muscles; spasticity or flaccidity of the oral facial muscles; and hypokinetic speech. Some common etiologies for dysarthria in children include stroke, brain tumor, aneurysm, traumatic brain injury (TBI), encephalopathy, seizure disorder, cerebral palsy (CP), and high-level SCI. Apraxia refers to a group of related motor speech disorders resulting from the impaired ability to produce movement in musculature in the absence of muscle weakness. TABLE 4.3 MOTOR SPEECH DISORDERS DEVELOPMENTAL ACQUIRED Developmental: no specific identifiable etiology to explain delays in speech acquisition Acquired: an adverse event (usually neurologic) occurs that impedes continuation of previously normal speech acquisition Phonological disorder Dysarthria Verbal apraxia Verbal apraxia Articulation disorder Articulation disorder Oral apraxia refers to an impairment of the voluntary ability to produce movements of the facial, labial, mandibular, lingual, palatal, pharyngeal, or laryngeal musculature in the absence of muscle weakness. Verbal apraxia (also called apraxia of speech, or AOS) refers to an impairment of motor speech characterized by a diminished ability to program the positioning and sequencing of movements of the speech musculature for volitional production of speech sounds. Verbal apraxia may result in perceptual disturbances of breathing/speaking synchrony, articulation, and prosody. Verbal apraxia is an acquired diagnosis related to an injury or illness. The site of lesion is generally the left precentral motor or insular areas. Developmental verbal apraxia (also called developmental apraxia of speech, or DAOS) refers to a speech disorder resulting from delays or deviances in those processes involved in planning and programming movement sequences for speech. Associated characteristics of DAOS include receptive-better-than-expressive language, presence of oral apraxia (may or may not exist with DAOS), phonemic errors (often sound omissions), difficulty achieving initial articulatory configuration, increase in errors with increase in word length and/or phonetic complexity, connected speech poorer than word production, inconsistent error patterns, groping and/or trial-and-error behavior, and presence of vowel errors. DAOS is not related to a specific identifiable lesion and is defined primarily by speech symptoms. Children with motor speech disorders may demonstrate impaired phonological systems because their ability to acquire the sound system of their language is believed to be undermined by difficulties in managing the intense motor demands of connected speech (9). COMPONENTS OF SPEECH AND LANGUAGE With regard to models of language, the prevailing school of thought follows Bloom and Lahey’s philosophy, which proposes three main components of language: form, content, and use (Figure 4.4). According to Bloom and Lahey, language can be defined as “a knowledge of a code for representing ideas about the world through a conventional system of arbitrary signals for communication (10).” These three components can be subdivided further into phonology, morphology, syntax, semantics, and pragmatics, as described in the following sections. Form Form with reference to language refers to the rule-based structure humans employ to formulate language, ranging from phonemes to sentences, and comprises phonology, morphology, and syntax. Phonology refers to the rule-governed system by which sounds, or phonemes, are combined to create meaningful units, or words. The English language contains 44 recognized phonemes, which are classified as consonants or vowels. This distinction involves the presence or absence of interruption of the airstream. Vowels are formed through modulation (without interruption) of the airstream via variation in position of the lips and tongue (Figure 4.5) (11). FIGURE 4.4 The three components of language. Variations in tongue position for production of different vowels are systematically characterized as high, mid, or low, as well as front, central, or back, and can further be described as tense or lax (Figure 4.6) (12). For example, the vowel /i/, pronounced “ee,” is considered a high, front, tense vowel, as the front of the tongue is high and the tongue is tensed. Diphthongs are combinations of vowels, and require movement of the tongue from one position to another during production. FIGURE 4.5 Vowel areas. FIGURE 4.6 Tongue positions for vowel production. Source: Reprinted with permission from Ref. (12). Bronstein AJ. The Pronunciation of American English. New York, NY: Appleton-Century-Crofts, Inc., 1960. Consonants are formed through a combination of varying degrees of interruption of the airstream and variations in tongue and lip posture (see Figure 4.3). Phonemic acquisition in children follows a systematic sequence, and it is believed that children acquire phonemes not in isolation, but rather in the context of their relationship to other sounds in a word (Table 4.5) (13). TABLE 4.5 PHONEMIC ACQUISITION: AGE AT WHICH 75% OF CHILDREN TESTED CORRECTLY ARTICULATED CONSONANT SOUNDS AGE (YEARS) SOUNDS 2 m, n, h, p, η 2.4 f, j, k, d 2.8 w, b, t 3 g, s 3.4 r, l 3.8 š (she), tš (chin) 4 ð (father), Z (measure) 4+ dž (jar), θ (thin), v, z Source: Adapted from Ref. (13). Soifer, LH. Development and disorders of communication. In: Molnar GE, ed. Pediatric Rehabilitation. 2nd ed. Baltimore, MA: Lippincott, Williams & Wilkins;1985. TABLE 4.6 ACQUISITION OF CONSONANT SOUNDS Table 4.6 provides a graphic representation of the typical age ranges during which most children acquire consonant sounds (14,15). This is useful in determining at what age a child is considered outside of the norm for acquisition of a specific sound and when intervention might be indicated. With regard to how well one can expect to understand a child’s speech over the course of phonemic acquisition, Lynch et al. provide an estimate of speech intelligibility at different ages, summarized in Table 4.7 (16). Phonological disorders are a subset of sound production disorders in which linguistic and cognitive factors, rather than motor planning or execution, are thought to be central to observed difficulties (common etiologic variables include otitis media with effusion, genetics, and psychosocial involvement) (17). Developmental phonological disorders result when children fail to progress in their acquisition of specific phonemes. The currently accepted theory regarding phonology in children proposes the existence of phonological processes that are present in the phonological systems of all children as they develop language, and are systematically eliminated at predictable ages in a standard developmental progression. Failure to eliminate, or resolve, these processes, results in a phonological processing disorder. An example of a developmental phonological process is “stopping of fricatives,” in which a child systematically substitutes a stop sound (a sound that stops airflow, such as /p, t, k/) for a fricative sound (a sound that produces friction through partial interruption of airflow, such as [th, s, z, f, v]), producing words such as “dum” for “thumb,” “tun” for “sun,” or “dip” for “zip.” These sound substitutions are systematic and applied by the child in the same context each time that sound occurs. Nondevelopmental phonological processes are indicative of disordered versus delayed phonological development, and are rarely seen in normal development. An example of a nondevelopmental phonological process is initial consonant deletion, in which a child deletes the initial sound in a word, such as “ee”/”key” or “ake”/”make.” TABLE 4.7 SPEECH INTELLIGIBILITY IN CHILDREN By 18 months, a child’s speech is normally 25% intelligible. By 24 months, a child’s speech is normally 50%–75% intelligible. By 36 months, a child’s speech is normally 75%–100% intelligible. Source: Adapted from Ref. (16). Lynch JI, Brookshire BL, Fox DR. A Parent-Child Cleft Palate Curriculum: Developing Speech and Language. Oregon: CC Publications;1980:102. Table 4.8 illustrates the typical developmental sequence for resolving phonological processes (18). TABLE 4.8 RESOLUTION OF PHONOLOGICAL PROCESSES: AGES BY WHICH PHONOLOGICAL PROCESSES ARE ELIMINATED PHONOLOGICAL PROCESS EXAMPLE GONE BY APPROXIMATELY (YEARS; MONTHS) Context sensitive voicing pig = big 3; 0 Word-final devoicing pig = pick 3; 0 Final consonant deletion comb = coe 3; 3 Fronting car = tar ship = sip 3; 6 Consonant harmony mine = mime kittycat = tittytat 3; 9 Weak syllable deletion elephant = efant potato = tato television = tevision banana = nana 4; 0 Cluster reduction spoon = poon train = chain clean = keen 4; 0 Gliding of liquids run = one leg = weg leg = yeg 5; 0 Stopping /f/ fish = tish 3; 0 Stopping /s/ soap = dope 3; 0 Stopping /v/ very = berry 3; 6 Stopping /z/ zoo = doo 3; 6 Stopping “sh” shop = dop 4; 6 Stopping “j” jump = dump 4; 6 Stopping “ch” chair = tare 4; 6 Stopping voiceless “th” thing = ting 5; 0 Stopping voiced “th” them = dem 5; 0 Source: Adapted from Ref. (18). Bowen C. Developmental Phonological Disorders: A Practical Guide for Families and Teachers. Melbourne: ACER Press;1998. Disorders affecting morphology are most typically developmental and result when children have difficulty mastering the acquisition of rules for applying morphological markers. Difficulty with use of morphological markers can also be seen following certain types of focal brain injury, such as damage to Broca’s area, when expressive language becomes telegraphic in nature, losing the nuances provided by morphological markers. Syntax refers to the system of rules by which words are combined to create phrases, clauses, and sentences. The various parts of speech in English (eg, nouns, pronouns, verbs, adverbs, adjectives, etc.) serve different functions within these constructions, such as description, action, and attribute, and as such have specific rules for combination with each other. For example, the basic word order in English is subject–verb–object. As with morphology, disorders affecting syntax are typically developmental and are the result of difficulty mastering the acquisition of rules for creating grammatically correct sentences. Content Content with reference to language refers to the semantics, or meaning, of words, as they relate to, or represent, objects, actions, and relationships. Semantics, or meaning, is conveyed through the use of words or other symbols within a given context. Development of semantics in children reflects growing and changing concepts related to experiences, culture, and cognitive level. An example of a changing semantic notion is that of overgeneralization. Children first learn the meaning of a word based on one representation of that word and initially overgeneralize it to apply to all similar representations. Hence, “dog” may at some point be applied to denote all four-legged creatures. Child language disorders affecting semantics may be developmental and related to general cognitive development, or they may be acquired. Examples of disorders that involve semantics include specific language impairment (SLI), semantic–pragmatic language disorder, and Landau–Kleffner syndrome (19). In all these cases, children exhibit some degree of difficulty understanding the meaning of words and sentences. For children with semantic processing difficulties, the more abstract a concept is, the more difficult it is to understand. This holds true for things that require interpretation beyond the literal meaning, such as might be required in idioms or slang expressions. Deficits related to semantics can also result in difficulty identifying the key points in a sentence or story, which in turn may lead to problems with topic maintenance. Use Use with reference to language describes the function language serves within a social context, and is governed by pragmatics. Pragmatics refers to how we use the language we have acquired to communicate in social situations. Within a social interaction, language may be used in many different ways, such as to make comments, to ask questions, to acknowledge comments, and to answer questions. In 1976, Elizabeth Bates described three critical components of pragmatics: the ability to use speech acts to express intentionality in order to accomplish a given purpose (function), the ability to use social understanding and perspective-taking ability to make presuppositional judgments, and the ability to apply rules of discourse (eg, quantity, quality, relevance, clarity) in order to engage in cooperative conversational exchanges (20). Child language disorders affecting pragmatics are most typically those associated with disorders on the autism spectrum. Recent changes presented in the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) include a new diagnosis separate from autism spectrum disorder termed social communication disorder (SCD). This disorder is characterized by the presence of deficits in social communication that cannot be explained by cognitive impairment (21). Acquired injuries that may have an impact on pragmatics include TBI affecting the frontal lobes. Frontal lobe injury often impairs executive functioning and increases impulsivity, resulting in impaired judgment. This, in turn, may impair one’s ability to understand perspective and to apply rules of discourse appropriately. To summarize, language competence requires the successful intersection of form, content, and use. As simple as it may seem, having a successful conversation is a complex act requiring integration of many aspects of language and involving a blending of linguistic features with sociocultural understandings. “Conversation is not a chain of utterances, but rather a matrix of utterances and actions bound together by a web of understandings and reactions” (21). SPEECH AND LANGUAGE ACQUISITION Acquisition of speech and language skills follows a fairly systematic progression, with easily identifiable milestones associated with specific ages in each area, as briefly outlined here (22,23). • Birth to 3 months • 6 to 12 months • 12–18 months • 18 to 24 months • 2 to 3 years • 3 to 4 years • 4 to 5 years • 5 to 6 years • 6 to 7 years
 Makes pleasure sounds such as cooing
Makes pleasure sounds such as cooing
 Develops differential cries for different needs
Develops differential cries for different needs
 Develops social smile
Develops social smile
 Increase in variety of vocalizations
Increase in variety of vocalizations
 Babbling sounds more speech-like, with increased consonant productions
Babbling sounds more speech-like, with increased consonant productions
 Uses sounds and gestures to indicate wants
Uses sounds and gestures to indicate wants
 Reduplicative babbling occurs (eg, dada, bibi, etc.)
Reduplicative babbling occurs (eg, dada, bibi, etc.)
 Uses speech sounds to get attention
Uses speech sounds to get attention
 First words emerge (~10–12 months)
First words emerge (~10–12 months)
 Responds to simple requests
Responds to simple requests
 Imitates speech sounds
Imitates speech sounds
 Imitates words overheard in conversation
Imitates words overheard in conversation
 Names familiar objects on request
Names familiar objects on request
 Follows one-step commands during play
Follows one-step commands during play
 Finds a familiar object not in sight
Finds a familiar object not in sight
 Uses words more frequently than jargon
Uses words more frequently than jargon
 Has expressive vocabulary of 50 to 100 words
Has expressive vocabulary of 50 to 100 words
 Has receptive vocabulary of 300+ words
Has receptive vocabulary of 300+ words
 Uses two- to three-word sentences
Uses two- to three-word sentences
 Points to pictures in books
Points to pictures in books
 Speech is understood by familiar listeners most of the time
Speech is understood by familiar listeners most of the time
 Uses simple sentences with negatives, imperatives, and questions
Uses simple sentences with negatives, imperatives, and questions
 Talks about activities at school and home
Talks about activities at school and home
 Understands simple “wh-” question words
Understands simple “wh-” question words
 Mean length of utterance (MLU) = 4.6 to 5.7 words
Mean length of utterance (MLU) = 4.6 to 5.7 words
 Uses grammatically correct sentences
Uses grammatically correct sentences
 Relays a long story accurately
Relays a long story accurately
 MLU = 6.6 words
MLU = 6.6 words
 Uses all pronouns consistently
Uses all pronouns consistently
 Comprehends 13,000 words
Comprehends 13,000 words
 MLU = 7.3 words
MLU = 7.3 words
 Comprehends 20,000 to 26,000 words
Comprehends 20,000 to 26,000 words
 Refines syntax
Refines syntax
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


