3 Kinematics and coupled motion of the spine
Clinicians use palpatory assessment of individual intervertebral segments prior to the application of a thrust technique. The osteopathic profession has used Fryette’s model of the physiological movements of the spine to assist in the diagnosis of somatic dysfunction and the application of treatment techniques. Fryette1 outlined his research into the physiological movements of the vertebral column in 1918. He presented a model that indicated coupled motion occurred in the spine and displayed different coupling characteristics dependent upon spinal segmental level and posture. The muscle energy approach is one system of segmental spinal lesion diagnosis and treatment predicated upon Fryette’s Laws.2 Practitioners utilizing muscle energy technique (MET) use these laws of coupled motion as a predictive model both to formulate a mechanical diagnosis and to select the precisely controlled position required in the application of both muscle energy and thrust techniques. Current literature challenges the validity of Fryette’s Laws.
Biomechanics
In the clinical setting, vertebral motion is described using standard anatomical cardinal planes and axes of the body. Spinal motion can be described as rotation around, and translation along, an axis as the vertebral body moves along one of the cardinal planes. By convention the vertical axis is labelled the y-axis; the horizontal axis is labelled the x-axis; and the antero-posterior axis is the z-axis (Fig. 3.1).3
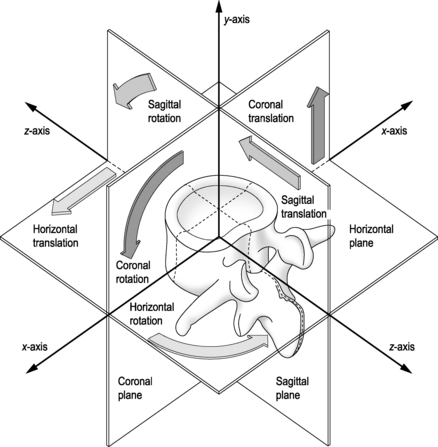
In biomechanical terms, flexion is anterior (sagittal) rotation of the superior vertebra around the x-axis, while there is accompanying forward (sagittal) translation of the vertebral body along the z-axis. In extension, the opposite occurs and the superior vertebra rotates posteriorly around the x-axis and translates posteriorly along the z-axis. In sidebending, there is bone rotation around the antero-posterior z-axis, but sidebending is rarely a pure movement and is generally accompanied by vertebral rotation. The combination, and association, of one movement with others is termed ‘coupled motion’. The concept of coupled motion is not recent. As early as 1905, Lovett4 published his observations of coupled motion of the spine.
Coupled Motion
Coupled motion is described by White and Panjabi5 as a ‘phenomenon of consistent association of one motion (translation or rotation) about an axis with another motion about a second axis’. Bogduk and Twomey3 describe coupled movements as ‘movements that occur in an unintended or unexpected direction during the execution of a desired motion’. Stokes et al6 simply state coupling to be when ‘a primary (or intentional) movement results in a joint also moving in other directions’. Where rotation occurs in a consistent manner as an accompaniment to sidebending it has been termed conjunct rotation.7,8 Therefore, in rotation the vertebra should rotate around the vertical y-axis but translation will be complex dependent upon the extent and direction of coupling movements. Coupling will cause shifting axes of motion.
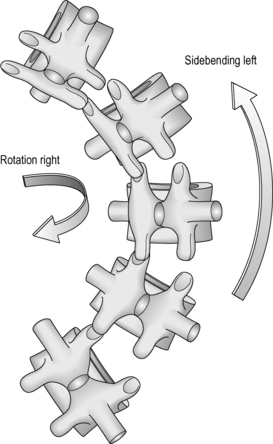
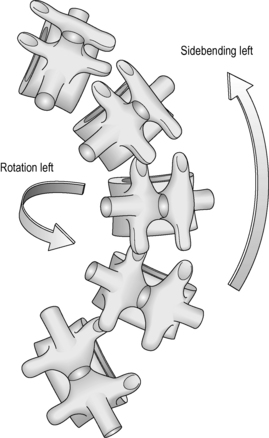
Greenman9 maintains that rotation of the spinal column is always coupled with sidebending with the exception of the atlanto-axial joint. The coupled rotation can be in the same direction as sidebending (e.g. sidebending right, rotation right) or in opposite directions (e.g. sidebending right, rotation left). The osteopathic profession developed the convention of naming the coupled movements as Type 1 and Type 2 movements (Figs. 3.2 and 3.3).10
Fryette acknowledged that Lovett’s findings for the thoracic and lumbar spine were correct in the position Lovett had placed the spine for his cadaveric experiments, but maintained they would not be true if the lumbar and thoracic spine were placed in different positions of flexion or extension. Fryette performed his own experiments upon a ‘spine mounted in soft rubber’ and introduced the concept of neutral (facets not engaged) and non-neutral (facets engaged and controlling vertebral motion) positioning. Fryette defined neutral ‘to mean the position of any area of the spine in which the facets are idling, in the position between the beginning of flexion and the beginning of extension’. In the cervical spine below C2, the facets are considered always to be in a non-neutral position and are therefore assumed to control vertebral motion. The thoracic and lumbar regions have the possibility of neutral and non-neutral positioning. Mitchell2 summarizes Fryette’s Laws as follows:
Fryette’s Laws
• Law 1. Neutral sidebending produces rotation to the other side or, in other words, the sidebending group rotates itself toward the convexity of the sidebend, with maximum rotation at the apex.
• Law 2. Non-neutral (vertebra hyperflexed or hyperextended) rotation and sidebending go to the same side, individual joints acting at one time.
• Law 3. Introducing motion to a vertebral joint in one plane automatically reduces its mobility in the other two planes.
Research into coupled movement has been undertaken on cadavers and live subjects. Cadaver research has allowed precise measurements to be taken of coupling behaviour, but has the disadvantage of being unable to reflect the activity of muscles or the accurate effects of load on different postures. Plain radiography has been superseded by the more accurate biplanar radiographic studies that allow research to be undertaken under more normal physiological conditions. Most research has been performed on the lumbar spine.
Reviews of the literature conclude that coupled motion exists but there is conflicting evidence as to the specific characteristics of coupled motion.11–14 Many authors have demonstrated a coupling relationship between sideflexion and rotation8,15–29 but there is inconsistent reporting of the direction of coupling.30 Other authors maintain that sidebending and rotation are purely uniplanar motion occurring independently of each other.31,32
Cervical spine (Fig. 3.4)
Stoddard15 demonstrated radiologically that sidebending in the cervical spine is always accompanied by rotation to the same side regardless of cervical posture. Stoddard’s observations in relation to the cervical spine are consistent with Lovett’s findings and Fryette’s Laws. These findings are further supported by research undertaken using biplanar X-ray analysis20 and stereophotogrammetry.24 In 20 normal male volunteers, when the head was rotated, lateral bending occurred by coupling in the same direction at each segment below the C3 vertebra. Interestingly coupling was not restricted to lateral bending. At the same time, flexion took place by coupling at each segment below the C5–6 vertebra and extension above the C4–5 level. In a study of active range of motion in the cervical spine during daily functional tasks, Bennett et al25 noted that the normal coupling pattern for the cervical spine is rotation and sidebending to the same side. Three-dimensional magnetic resonance imaging (MRI) confirms that the coupling of lateral bending and axial rotation was in the same direction in the cervical spine below C2.27 Malmstrom et al26 confirmed this coupling behaviour in asymptomatic subjects up to the age of 70 with decreasing coupling in all cardinal planes with increasing age. Elderly subjects (70–79 years of age) exhibited a change in coupling behaviour with rotation being coupled with contralateral lateral flexion.

Craniocervical junction (Fig. 3.5)
The anatomy of the upper cervical spine differs significantly from the cervical spine below C2. Coupling behaviour has been reported in relation to the upper cervical spine24,33–35 but has not been as extensively investigated as in other regions of the spine. Stereophotogrammetry revealed consistent coupling of axial rotation and lateral bending to the opposite side at C0–1 and C1–2 and vice versa.24 Three-dimensional MRI confirmed the relationship between axial rotation and lateral bending to the opposite side.35 This is the reverse of the coupling behaviour in the cervical spine below C2.

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


