Closed Kidney Injury
Tracey A. Viola, DO, Family Practice and Sports Medicine, Lake Placid Health Center, 29 Church Street, Lake Placid, NY 12946, USA. E-mail address: tracey.viola@gmail.com
Keywords
Blunt renal trauma
Kidney
Trauma
Injury
AAST organ injury scale
Introduction
It has been estimated that, every year, children under the age of 18 account for 30 million emergency room visits, and 7.5 million of these are due to trauma.1 Trauma is the leading cause of death in children.2,3 The most common causes of trauma in pediatrics are falls and motor vehicle accidents (MVA).1,4,5
The prevalence of renal injury in blunt trauma ranges from 1%,6 1.4% to 3.25%,7 10%,8 and 10% to 20%,5 and the kidney is the most common urologic injury.8–11 Between 80% and 90% of all renal injuries are due to a blunt mechanism,6–8 and in children 90% are caused by blunt trauma.4,5 With a blunt injury, either the ribs or the abdominal organs hit the kidneys.7 Most isolated renal injuries, 95% to 98%, are minor and conservatively treated. Penetrating injuries make up 10% to 20% of injuries and are typically a gunshot or stab wound.8 The focus of this article is on closed renal injury; therefore, penetrating injury is not discussed.
Epidemiology of renal injury has been described from retrospective reviews. In an analysis of the National Trauma Data Bank, from 1994 to 2003, Kuan and coworkers found that boys and men account for 73.8% of renal injuries, and 74.2% of these are in people less than 40 years old.6 Santucci and colleauges’ consensus statement estimates the mean age is 20 to 30 years.7 In adults, MVA is the most common cause of renal injury.5,8
In regard to sports, both organized and recreational, contact and noncontact, sports have been associated with renal injury, although injury is rare overall. Almost all sports-related injuries are blunt11 and are caused by blunt abdominal or flank injury, rapid deceleration, or high-velocity impacts caused either by objects that are part of the sport or by high-speed sports.5
Wan and colleagues12 looked at the National Pediatric Trauma Registry from 1990 to 1999 and described injuries related to contact sports. Of a total of 81,923 trauma cases, only 5439 (6.64%) were due to sports in school-age children, and only 459 were abdominal or testicular (0.56% of all reported) injury. No injury resulted in functional loss of kidney. Although 62% of kidney injuries were related to football, other sports included baseball, basketball, hockey, and soccer. McAleer and colleagues13 reviewed their trauma registry from July 1984 through December 2000 and found only 6 renal injuries were caused by team sports. Rates of renal injury were as follows, in decreasing frequency: bicycling (27.6%), falls (23.5%), all-terrain vehicle riding (8.2%), playground (8.2%), motorcycling (6.1%), team sports (6.1%), skateboarding (6.1%), rollerblading (6.1%), playing ball (4.1%), equestrian sports (3.1%), and trampoline jumping (1%). No kidneys were lost in this series. Wu and Gaines report similar findings from another pediatric trauma database, in which contact and organized sports had less significant renal injury than dirt bikes, all-terrain-vehicle rollovers and riding, and bicycles.14
Many of the trauma databases are descriptive of urban populations, so Lloyd and colleagues15 studied adults at the Vail Valley Medical Center, Vail, CO. They specifically excluded MVAs and found that 85% of renal injuries were related to snow sports. These patients had different injury patterns than previously described in the urban population, fewer associated injuries, and less hypotension.
Patient history
As described earlier, the most common mechanism for renal injury is blunt trauma. The kidney is protected posteriorly by the ribs and back muscles, and anteriorly by the abdominal organs.7 Rapid deceleration injuries, for example, a fall or MVA, can also be significant because the renal hilum (pedicle and pyleoureteral junction) is fixed, and great forces are transmitted through this fixed area,4,7,9 with risk of vascular and uteropelvic junction injuries.4,7 Therefore, the history of the injury is important in risk-stratifying patients.
Another important factor in the history of injury is the age of the patient. There is thought that children are more likely to sustain renal trauma than their adult counterparts. Explanations such as greater size of kidney compared with the body, less perirenal fat to cushion the kidney, weaker abdominal muscles, and less protection from ribs, resulting in transmission of greater forces, have been postulated.2,4,5,7 In a retrospective review of 34 pediatric and 35 adult blunt renal trauma victims, Brown and coworkers found that although children were more likely to sustain major (grade IV or V) renal injury, they had lower overall injury severity scores (a scale that describes multiple injuries). The most common mechanism of injury in children was falls (44%), and in adults the most common mechanism of injury was MVA (80%) in this series.2
Physical examination
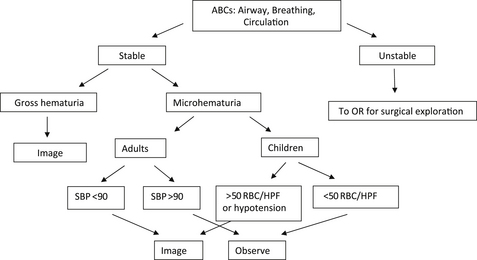
In the triage of any trauma patient, initial assessment should include the ABCs (airway, breathing, and circulation with pulse and blood pressure measurements). Hemodynamic instability in children or adults, not responsive to resuscitation efforts, should be surgically explored (Fig. 1 shows the assessment algorithm).4,5,9 If the patient is stable, a secondary survey should be performed next. Of note, whereas in adults blood pressure is an adequate assessment of volume status,4 in children, it is not, as they can be normotensive and hypovolemic.4,5
On examination, special attention should be paid to signs that indicate a renal injury. Objective signs include gross hematuria,4,5 flank hematoma,5,7,9 flank5,7,16 or abdominal eccymoses4 or tenderness,4,5,9,16 pelvic pain,4 rib fractures or pain,4,5,7,9,16 transverse process pain,16 penetrating injuries,5,9 or abdominal examination with peritoneal signs (rebound tenderness, guarding).16
After examination, urinalysis should be performed.5,16 The most common laboratory finding is microscopic hematuria,5 and 80% to 95% of significant renal injuries in adults do present with hematuria.7,8 If microscopic hematuria is present, quantification can help determine if further imaging is indicated. Predictors of significant renal injury in adults include microscopic hematuria and hypotension,5,7,9 and in children predictors of significant renal injury include greater than 50 red blood cells (RBCs) per high-power field and should be further imaged.4,5,7 Of importance, the presence or absence and number of RBCs do not necessarily correlate to injury.4,7,9 For example, with a deceleration injury, there may not be hematuria despite pedicle injuries.9 If gross hematuria is noted, further imaging should be performed.5,16
Additional laboratory evaluation should include complete blood count, complete chemistry including electrolytes, creatinine, glucose, liver function tests, amylase, and lipase5,16 to evaluate for other abdominal organ injury. Radiographs can be helpful in the evaluation of rib and transverse process fractures.16
Serial examinations, including vital signs, abdominal examinations, and hematocrit, are also important in the ongoing care of renal injury.4,5 If no imaging is necessary, Santucci and colleagues7 recommend observation and a follow-up urinalysis in 3 weeks.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


