Intra-operative Skull-Skeletal Traction
Stephen J. Lewis
So Kato
With the advent of pedicle screw instrumentation, improved corrections have been achieved in the treatment of coronal plane deformities. However, in larger, stiffer curves, or in patients with small or absent pedicles, screws alone may not be sufficient to achieve the desired correction.
Traction has long been used as an adjunct in the treatment of scoliosis (1). Preoperative and intraoperative tractions have been part of the original treatment. Even Dr. Dubousset used intraoperative traction during his original corrections with CD instrumentation (2). In this chapter, a summary of the indications, techniques, and limitations of the use of intraoperative skull-skeletal traction in the treatment of pediatric coronal plane deformities will be reviewed.
ROLE OF TRACTION
The use of intraoperative skull-skeletal traction provides initial correction to the curve prior to incision. Depending on the weight used, the magnitude of the coronal Cobb angle can decrease by 50% compared to the preoperative standing film (3, 4, 5). This significant reduction in the curve can expedite spine exposure, provide derotation and translation to the curve facilitating screw insertion, and aid in the correction of the deformity and rod placement. While bilateral femoral traction is used in cases with a level pelvis (Fig. 48-1A), in the presence of pelvic obliquity, unilateral traction (Fig. 48-1B) on the high pelvic side can be used to level the pelvis (6, 7).
With the traction in place, standard curve correction techniques can be utilized to further correct the deformity. The traction is placed just prior to flipping the patient onto the operating room table after the anesthetic induction has been completed. Once the rods are inserted and the correction is completed, the weight of the traction is removed. The pins are removed in the operating room at the conclusion of the case prior to the patient being awakened from the anesthesia.
INDICATIONS
While intraoperative traction can be used as an adjunct in all cases of scoliosis, the best indications for its use include
Nonfused coronal plane deformities greater than 75 degrees
Coronal plane deformities with small or absent pedicles
Neuromuscular deformities with pelvic obliquity
Larger curves often need greater release to achieve the desired correction (Fig. 48-2A-C). While this flexibility can be achieved through anterior releases or posterior column osteotomies, the traction can provide significant correction (Fig. 48-2D) so that these releases can be either avoided or limited to just one or two levels (Fig. 48-2F, G) around the apex (8, 9, 10, 11, 12).
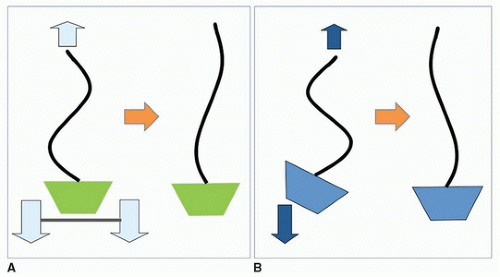 FIGURE 48-1 (A) is a schematic of bilateral traction used in cases of scoliosis without pelvic obliquity. Bilateral traction with countertraction on the skull produces a symmetrical pull on the lower extremities providing correction to the spinal deformity. In cases of pelvic obliquity (B), unilateral femoral traction is placed on the leg with the high pelvis. With countertraction on the skull, unilateral pull on the femoral pin reduces the pelvic obliquity while correcting the spinal deformity. |
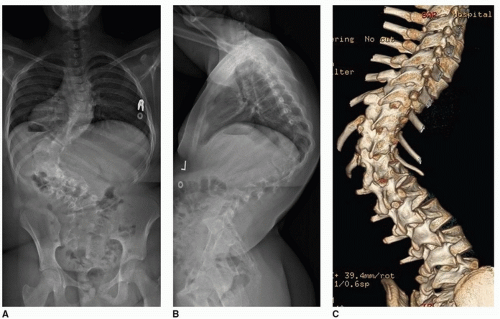 FIGURE 48-2 Long-cassette standing anteroposterior (A) and lateral (B) radiograph of a 14-year-old girl with a kyphotic idiopathic scoliosis. CT 3-dimensional reconstructions dorsal (C) and ventral (D) demonstrate the absence of any congenital anomalies. Significant reduction of the curve is obtained with intraoperative skull-skeletal traction (E). Following an apical Smith-Petersen osteotomy to obtain further release and a T4 to L4 construct, a well-balanced correction was obtained as demonstrated in the long-cassette standing anteroposterior (F) and lateral (G) radiographs. |
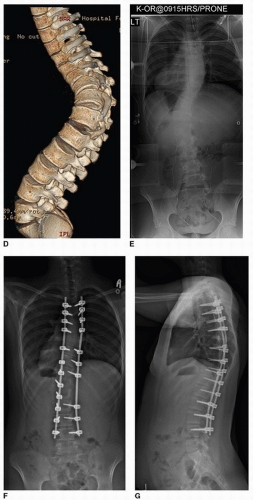 FIGURE 48-2 (Continued) |
Certain conditions, including Marfan syndrome and neurofibromatosis (Fig. 48-3A-E), often have small or absent pedicles. This is particularly prevalent around the apex of the deformity. Similarly, small pedicles are noted in thoracolumbar and lumbar idiopathic scoliosis curves, especially around the apex at L1 and L2. Traction in these cases (Fig. 48-3F) provides significant initial correction making it less necessary to obtain periapical fixation, with the inherent risk of medial or lateral pedicle screw breach (Fig. 48-4A-D).
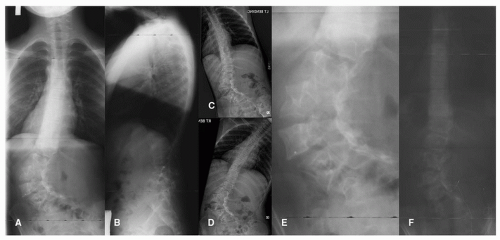 FIGURE 48-3 Long-cassette standing posteroanterior (A), lateral (B), left (C), and right (D) bender radiographs of a 10-year-old girl with neurofibromatosis with a sharp, progressive lumbar scoliosis. A magnified view of the lumbar spine (E) highlights the absent upper lumbar pedicles secondary to large dural ectasia. Using bilateral skull-femoral traction, a posteroanterior intraoperative radiograph (F) demonstrates correction of the translation, magnitude, and rotation of the main curve. |
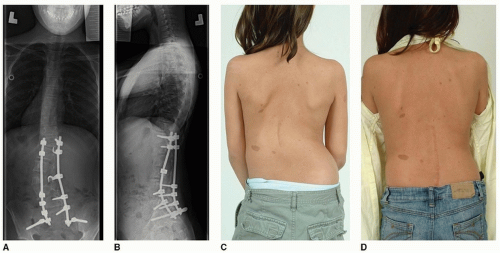 FIGURE 48-4 Postoperative standing posteroanterior (A) and lateral (B) radiographs of the patient presented in Figure 48-3. Preoperative (C) and postoperative (D) clinical views demonstrate cosmetic improvement in the translation and symmetry of her back. |
In the presence of pelvic obliquity, as seen in nonambulatory neuromuscular deformities (Figs. 48-5A, B




Related posts:






Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
