(1)
Department of Orthopedic Surgery Academic Medical Centre, University of Amsterdam, Amsterdam, The Netherlands
Abstract
The ankle joint was previously approached as a small joint only using small joint arthroscopy and small joint instruments. These days are over. The ankle joint should be considered as a major joint. Just like any other major joint, the pathology in the ankle joint can be safely treated with specific instrument of similar dimensions of those used on the knee and shoulder. In this chapter, the specific arthroscopic equipment for anterior ankle arthroscopy tendoscopy and the two-portal hindfoot approach are mentioned including arthroscopes, probes, graspers, and curettes. Current dedicated ankle arthroscopy sets contain instruments of appropriate dimensions, curvature, and size. This chapter gives an overview as well as my personal selection of instruments.
The ankle joint is a major joint.
Pathology in the ankle joint can be safely treated with specific instrument of similar dimensions of those used on the knee and shoulder.
A dedicated arthroscopy set contains a selection of instruments specifically designed for use in the ankle joint.
4.1 Arthroscopic Equipment
A 2.7-mm arthroscope with 30° obliquity and a length of 11 cm is routinely used for ankle arthroscopy. It can be applied with a 4.6-mm sheath or with a 2.9-mm sheath (Figs. 4.1 and 4.2). The 4.6-mm sheath has the advantage of a high-volume irrigation. The 2.0-mm sheath cannot deliver the same amount of irrigation fluid per time as the standard sheath. This is an important drawback when motorized instruments are used, as these cases benefit from an adequate amount of irrigation. For routine arthroscopic procedures such as anterior impingement syndrome, loose body removal, treatment of synovitis, and the vast majority of osteochondral defects, it is beneficial to use the 4.6-mm sheath. The 2.9-mm sheath can be used for treatment of osteochondral defects of the posterior talar dome (less than 8 % of all osteochondral defects in the ankle joint); pathology of the articular part of the tibiofibular joint (intrinsic syndesmosis), such as a soft tissue impediment or impregnated ossicles or loose bodies; posterior ankle problems that are treated by an anterior approach; and patients without a preoperative diagnosis.
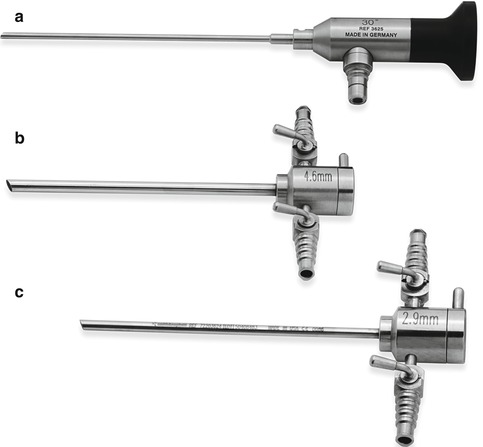

Fig. 4.1
(a) 2.7-mm arthroscope with 30° obliquity and a length of 11 cm. (b) Cannula 4.6 mm. (c) Cannula 2.9 mm (Courtesy of Smith & Nephew, Inc)
Fig. 4.2
2.7-mm arthroscope introduced in 4.6-mm cannula (Courtesy of Smith & Nephew, Inc)
4.2 Distraction
Routine joint distraction is not necessary to perform ankle arthroscopy. There are situations in which distraction helps to get access to a posterior osteochondral defect. A soft tissue distractor has been developed for better access to posterior lesions. The soft tissue distractor consists of the device which is shown in Fig. 4.3 and 6.5. This sterile strap is attached to a sterile belt which is placed around the waist of the surgeon. When the surgeon leans backwards, distraction of the ankle joint is obtained.

Fig. 4.3
Sterile ankle distractor foot strap (With kind permission of © Pau Golanó 2013)
4.3 Instrumentation
In the past, standard instruments that are used for knee or shoulder arthroscopy were used to perform ankle arthroscopy. However, the geometry of the ankle joint differs from the knee and shoulder joint. The ankle joint differs also in size. Basic instruments include a blade 11 knife, curved hemostatic forceps (mosquito), spinal needle and straight Kocher forceps (Fig. 4.4). The curved mosquito clamp is used for creating the portals, and a Kocher can be useful for removal of large bony fragments in case an arthroscopic forceps is too small.
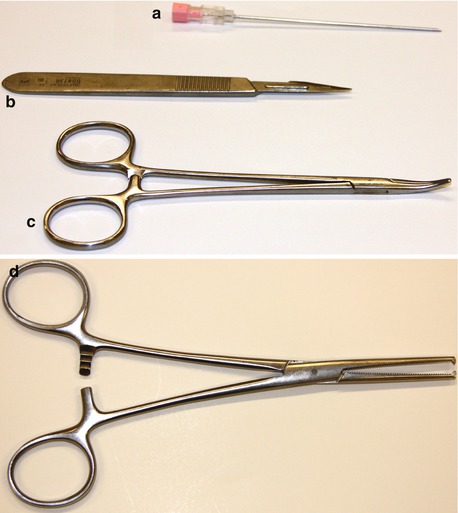
Fig. 4.4
(a) BD spinal needle 18GA 3.50 IN. (b) Scalpel handle no. 3 and blade no. 11, triangular blade with sharp point flat cutting edge parallel to the handle. (c) Leriche hemostatic forceps 15 cm curved (mosquito). (d) Dixon-Lovelace artery forceps 1 × 2T 16 (Kocher)
Dedicated ankle arthroscopy instrumentation sets have recently been developed. These sets contain instruments specifically designed to accommodate the geometry and size of the ankle joint.
4.4 Dedicated Ankle Arthroscopy Set
A dedicated arthroscopy set for ankle arthroscopy contains the following instruments: a straight 3.0-mm probe and a probe with a curved tip (Figs. 4.5 and 4.6). The curve accommodates palpating of structures in the posterior ankle joint since the curvature accommodates the curvature of the talus (Fig. 4.6). A calibration on the tip of the probe helps to measure the size of intra-articular structures as, for example, an osteochondral defect. A straight 4-mm osteotome is used for detachment of osteophytes, spurs, and bony ridges (Fig. 4.7).



Fig. 4.5
Smith & Nephew straight probe, 3 mm (Courtesy of Smith & Nephew, Inc)
Fig. 4.6
Smith & Nephew curved probe, 3 mm
Fig. 4.7
Smith & Nephew straight osteotome, 4 mm (Courtesy of Smith & Nephew, Inc)
In some instances, it helps to use a 3- or 4-mm osteotome with a 15° curvature as for removal of a posterior talar process (Fig. 4.8). The most useful instrument for detachment of ossicles is the curved elevator (Fig. 4.9). The curved elevator can also be used for removal of an os trigonum. For treatment of osteochondral defects, a 3-mm closed cup curette with a 15° curvature is most appropriate (Fig. 4.10). A 90° straight curette or curved curette (Fig. 4.11a, b) can also be used for this purpose. For microfracturing, chondro picks with different angles are available. A laser mark on the tip of the pick helps to determine the depth of the holes (Fig. 4.12a, b). Picks with a curved tip ease the access to posterior osteochondral talar defects (Fig. 4.13a, b ). For the 65° pick and 9° pick, a pick assist is available for hammering the device into dense subchondral bone (Fig. 4.14).










