Chapter 8 Injuries to the forearm bones
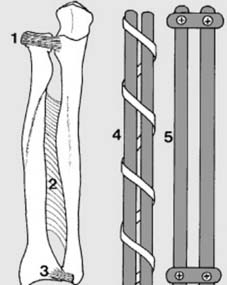
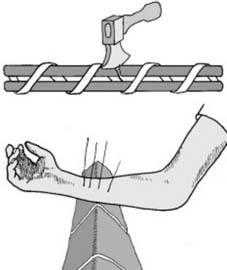
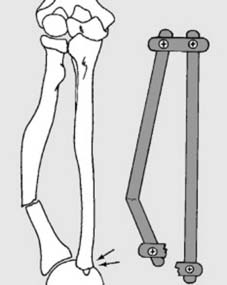
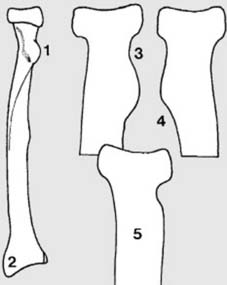
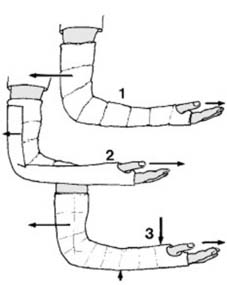
1 Anatomical features: The radius and ulna are bound together by (1) the annular (orbicular) ligament, (2) the interosseous membrane, (3) the radio-ulnar ligaments and the triangular fibrocartilage. This gives the radius and ulna some of the features of (4) a bundle of sticks and (5) a linked parallelogram.
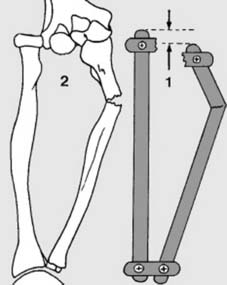
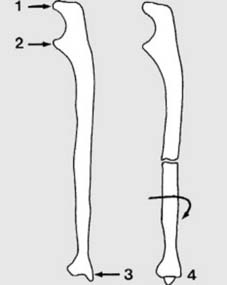
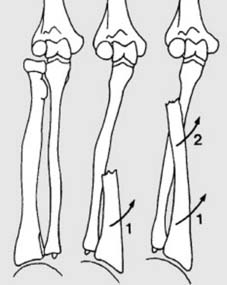
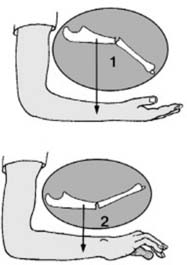
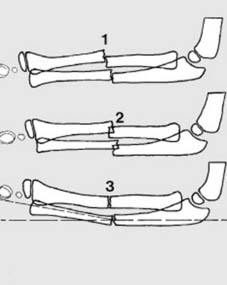
7 Axial rotation (b): Axial rotation of the ulna is rare, but always check to see that it is not present. To do so, note that in the lateral projection the olecranon (1), coronoid (2) and styloid process (3) should be clearly visible. This relationship is lost in the presence of axial rotation (4).
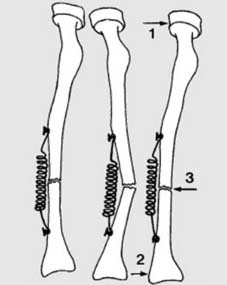

13 Fracture slipping (b): Another contributory cause of fracture slipping is when muscle wasting occurs in a patient in a full arm plaster wearing a collar and cuff sling. Loss of brachialis and brachioradialis bulk leads to plaster slackening and angulatory deformity. (Note: the soft tissue shadows in Frame 29) Patients with conservatively treated fractures should be given broad arm slings.


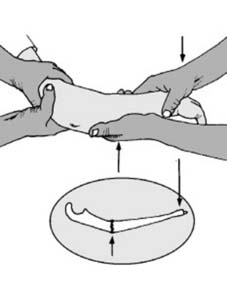
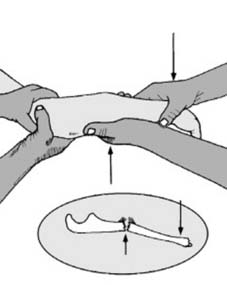

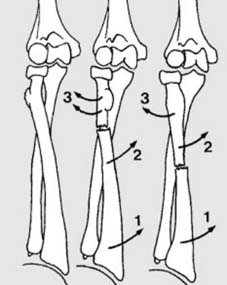
19 Treatment (d): Displaced fractures: These fractures are best dealt with under image intensifier control. When the fracture is displaced, axial rotation of the fragments should be looked for and the appropriate position in the pronation/supination range evaluated. The forearm is then placed in that position, and strong traction is applied for a quarter of a minute or so, with the patient well relaxed under a general anaesthetic. The elbow is flexed at a right angle for counter-traction.



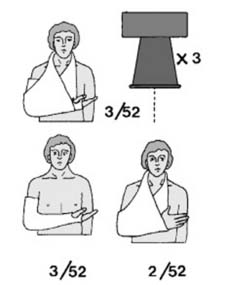
25 Treatment (i): Check the cast and the position of the fracture, preferably at weekly intervals, for 3–4 weeks; if satisfactory, the sling may then be discarded. Plaster fixation is maintained till union (usually after a further 3–4 weeks in a child of 10 years, and a further 1–2 weeks in a child of 4). The arm may be placed in a neutral position at 4 weeks if an extreme position was initially required. Thereafter mobilisation may be commenced from a sling.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


