Fig. 2.1
The radioulnar unity acts like a door with three locks. If only one lock is blocked, the whole door is blocked. If 2 locks are taken away, the door is unstable
Pathologies concerned by this stage are:
Fractures of the radial head, resection of the radial head, radial head prosthesis, and injuries of the annular and quadrate ligaments for the proximal lock
Fractures of the ulnar or radial diaphyses, isolated injuries of the interosseous membrane, considered rare, for the middle lock
Fractures of the distal ulnar or radial extremity that damage the distal radioulnar joint and injuries of the triangular complex for the distal lock
2.1.2 Stage 2 = 2 Locks Damaged
These damages concern the proximal and middle, middle and distal, or proximal and distal locks.
These injuries can block the radioulnar frame if 1 or 2 locks are blocked or destabilize it if both locks become unstable.
Pathologies concerned by this stage are:
Fracture of Monteggia that is an ulnar diaphyseal fracture combined with a dislocation of the proximal radioulnar joint. It’s an injury of the middle (the fracture tears the interosseous membrane) and proximal locks (Fig. 2.2).
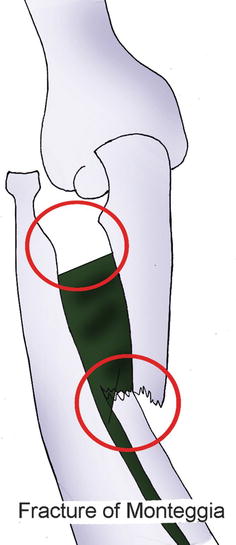
Fig. 2.2
Fracture of Monteggia combining an injury of the medium lock with one of the proximal locks
Fracture of Galeazzi that is a radial diaphyseal fracture combined with a dislocation of the distal radioulnar joint. It’s an injury of the middle (the fracture tears the interosseous membrane) and distal locks (Fig. 2.3).
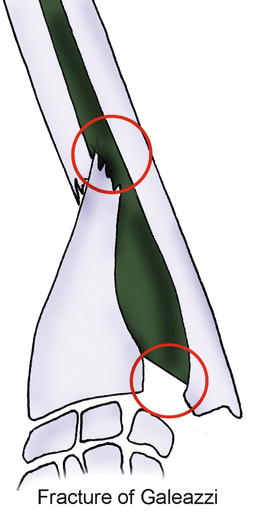
Fig. 2.3
Fracture of Galeazzi combining an injury of the distal lock with one of the medium locks
Crisscross injuries that are fractures of the radial head combined with dorsal dislocations of the ulnar head. They are injuries of the distal and proximal locks. The injury mechanism is a pivot of the two bones around an axis made by the middle part of the interosseous membrane (Fig. 2.4).
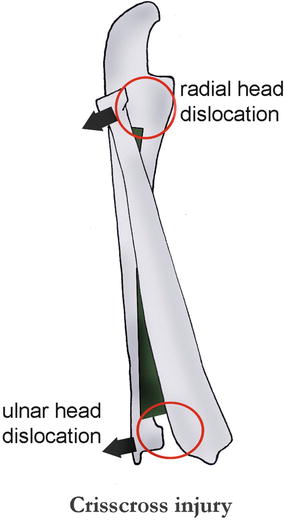
Fig. 2.4
Crisscross injury combining an injury of the distal lock with one of the proximal locks
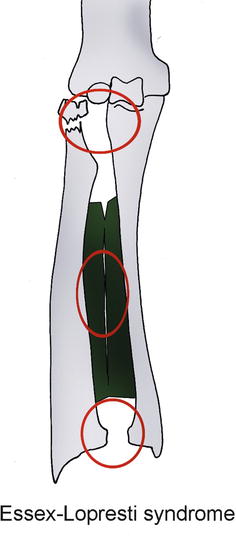
2.1.3 Stage 3 = 3 Locks Damaged
2.1.4 Physiopathology
At the physiopathological level, injuries of the radioulnar unity correspond to a fall with the wrist in extension. The grade of pronosupination during the fall defines the anatomical damages observed:
In total supination, fractures of the two forearm bones are frequent.
In 45° of supination, simple fractures of the radial head are more frequent.
In neutral position, Essex-Lopresti syndromes.
In pronation, complex fractures of the radial head.
These are tendencies and mustn’t be taken literally, as the exact position of the forearm during the trauma can be uncertain. Moreover, other components like the violence of the trauma have an important influence on the nature of the injuries.
2.2 Clinical and Paraclinical Signs
2.2.1 Clinical Signs [5]
It’s important to differentiate acute and old injuries. Chronic injuries are harder to treat; that’s why it’s important to make an early diagnosis. Symptoms vary depending on the number of damaged locks.
The limitation of mobility concerns pronosupination [3] and the different amplitudes of the elbow and wrist, and it can evolve with time: formation of a posttraumatic synostosis and inversion of the distal radioulnar index after resection of the radial head.
The natural evolution of an injury of the interosseous membrane is unknown as well as its healing mechanism. Echographies and MRIs have been realized to try to get more precise indications for surgery and stabilization of the forearm.
2.2.2 Paraclinical Signs
2.2.2.1 Static X-Rays
An injury of the interosseous membrane can be affirmed in case of lift of the radius, combined with dislocations of the proximal and distal radioulnar joints [6]. If the injury seems isolated, we have to look for an associated injury.
2.2.2.2 Dynamic X-Rays
They help highlighting proximal or distal instabilities. Ideally, this exam is realized under general anesthesia.
2.2.2.3 MRI
This exam is actually considered to be the gold standard. We visualize directly the interosseous membrane with hyposignal T1 and T2 and a sensitivity above 87 % according to some authors.
2.2.2.4 Echography
It’s an exam easily realized in case of emergency, but it has the disadvantage of being operator dependent. However, several authors say it has excellent sensitivity and specificity, which can be potentiated by a dynamic study of the interosseous membrane [6].
2.3 Therapeutic Process and Surgical Treatment
The treatment’s results will be worse in old injuries.
2.3.1 Osseous Surgery
A radial or ulnar fracture requires perfect reduction and osteosynthesis with plate to avoid any rotation or angulation disorders that would have an immediate impact on pronosupination and joint stability [7]. This perfect reduction will spontaneously produce a reduction of the dislocated joint.
2.3.2 Proximal Radioulnar Surgery
In fractures of Monteggia, the reduction of the ulnar fracture automatically reduces the dislocation of the radial head, except in case of imprisonment of the annular ligament, which requires a direct approach.
In fractures of the radial head, we’ll use osteosynthesis, looking for associated tears of the interosseous membrane, especially in comminuted fractures. In fractures of the radial head combined with a rupture of the interosseous membranes where we can’t keep the radial head, we’ll have to put a radial head prosthesis more or less associated to a ligamentoplasty of the interosseous membrane to decrease longitudinal constraints.
2.3.3 Distal Radioulnar Surgery
Reducing distal instabilities is usually done in supination. It can be maintained with a temporary radioulnar pin if the injuries are recent. The patients are often seen in chronic phase and we’ll have to surgically shorten the ulna. If they are in an even more advanced phase, we’ll realize less conservative procedures like the Sauve-Kapandji.
2.3.4 Interosseous Membrane Surgery
To repair the interosseous membrane, some authors have proposed ligamentoplasty techniques using the flexor carpi radialis tendon or the pes anserinus tendons with encouraging results [8].
2.4 Rehabilitation and Orthotic Treatment
Given the variety and complexity of the possible injuries, we won’t detail a precise rehabilitation protocol but rather elements to work with in order to regain a good functionality of the radioulnar unity [1, 9].
These elements concern the post-immobilization phase, after the damaged elements are solid and the pain and trophic disorders have disappeared.
They’re based on a global comprehension of the radioulnar unity [5, 10, 11], a “major” injury of one lock being possibly associated to a less important injury of another lock “hidden” during the paraclinical exam.
2.4.1 Mobility of the Radioulnar Unity
As seen in the Chap. 1, stiffness in one radioulnar lock blocks the whole radioulnar joint.
That’s why it’s essential to check the mobility of each radioulnar joint after any trauma in the forearm.
2.4.1.1 Distal Radioulnar Joint
It’s a trochoid joint with a cylindrical ulnar surface and a radial cavity.
Glidings between the ulna and radius must have amplitudes similar to those of the sane side, without cracking or snapping.
To maintain or regain good dynamics, these specific mobilizations must be realized in all the pronosupination amplitude.
The therapist is in front of the patient whose elbow is flexed.
He/she grabs the ulna and the internal part of the carpus with one hand and the radius and the external part of the carpus with the other.
The goal is to apply differential glidings between the radius and the ulna, maintained between the therapist’s thumbs and indexes (Fig. 2.6).

Fig. 2.6
Radioulnar mobilization technique. One hand does anteroposterior movements while the other realizes the opposite movement
2.4.1.2 Interosseous Membrane
Fibrosis in the interosseous membrane can also produce stiffness in the radioulnar unity.
Several techniques are used but their efficiency on the interosseous membrane has yet to be demonstrated.
Deep Massage
These techniques don’t have a direct effect on the membrane but can favor its mobilization, relaxing radioulnar muscles.
We use glided pressures, sanding, and palpating-rolling techniques.
Contraction-Stretching of the Muscles Inserted on the Interosseous Membrane
Alternating contractions and stretchings improves the local microcirculation (pumping effect), favors the fiber remodelling during the healing phase, and improves mobility in the different gliding planes.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


