Chapter 14 Injuries about the ankle
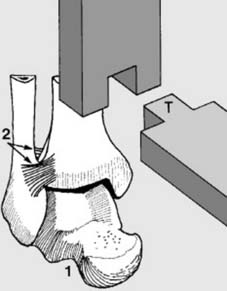
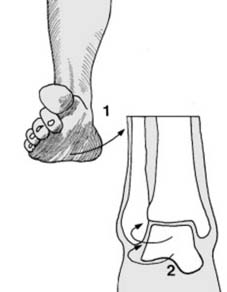
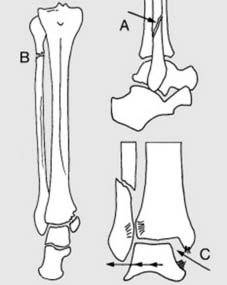
1 Anatomical considerations (a): The ankle joint is often fairly compared with the mortise and tenon joint of the woodworker. The talus (1) resembles the tenon (T), and is supported by the two malleoli and the articular surface of the tibia (the ankle mortise). The lateral malleolus is firmly attached to the tibia by the strong anterior and posterior tibiofibular ligaments (2).
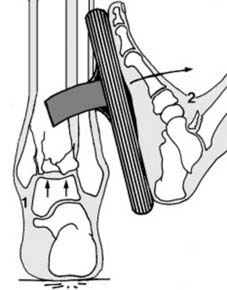
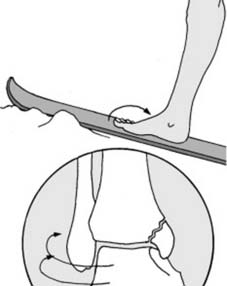
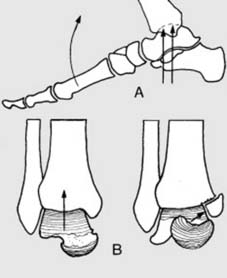
5 Mechanics of injury (b): External rotation of the talus may be produced in two different ways: 1. The foot may act as a long lever; any rotational force applied to the inside of the foot is transferred to the talus with a mechanical advantage as in any system of levers. Even greater leverage may occur if, for example, the foot is attached to a ski.



13 Pott’s classification of ankle fractures ctd: These fractures may be qualified by noting the presence of diastasis of the ankle or vertical compression.
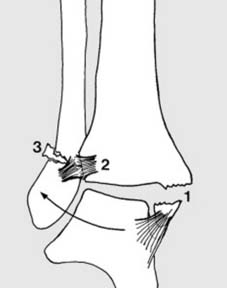
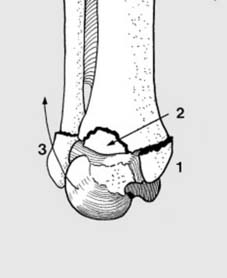
17 Supination/lateral rotation injuries (external rotation injury without diastasis) (a): The foot inverts (1). Due to the torque-converter principle, the talus rotates laterally in the ankle mortise (2). The ankle joint structures are thrown under stress and fail in a regular sequence. As each structure fails, the next is stressed. The number of structures involved is dependent on the magnitude of the forces applied to the joint.




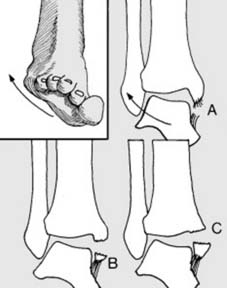
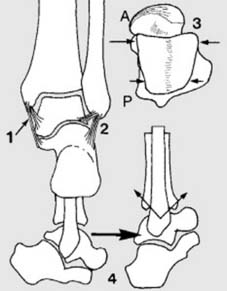
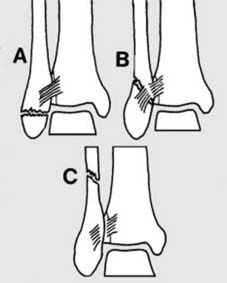
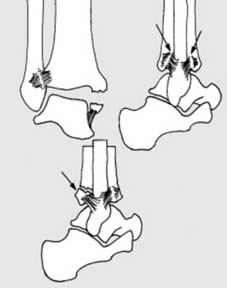
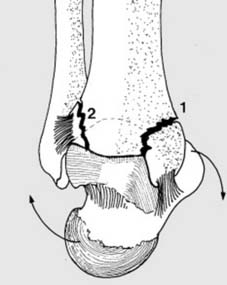
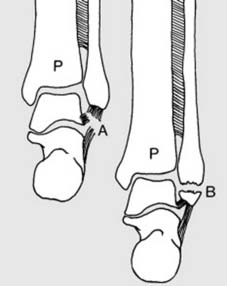
23 Pronation/abduction injuries (abduction injuries) (a): The foot everts and the talus swings into abduction. The first structures to be affected are on the medial side. Either (A) the deltoid ligament ruptures (rare) or there is an avulsion fracture of the medial malleolus. The fragment may be small (B) or large (C). In either case the fracture line runs horizontally.


27 Radiographs (b): In this Stage 3 abduction fracture, note the direction of talar tilting, the avulsion fracture of the medial malleolus with a large fragment and the distally-situated fibular fracture. The latter is not strictly horizontal, and its slightly spiral appearance suggests that there has been a rotational element. (As a first aid measure it would be normal practice to improve on this deformity (and that in Frame 33) to lessen the risks of skin necrosis on the medial side.)
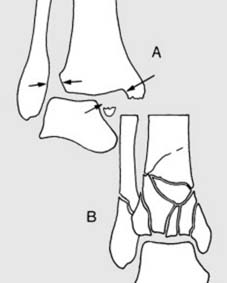
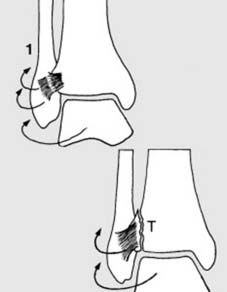
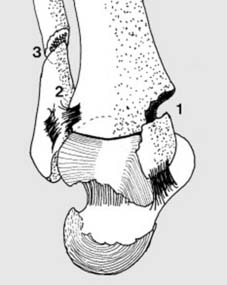
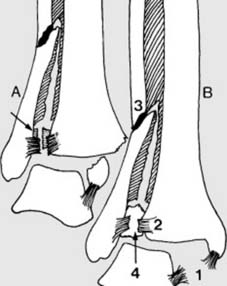
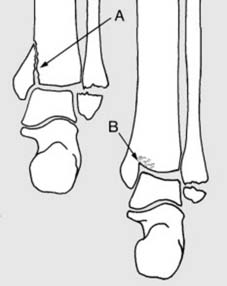
29 Pronation/lateral rotation (b): As the talus continues to twist, it impinges on the fibula. The anterior tibiofibular ligament is put under tension: in the second stage of P/L injuries, its tibial attachment is avulsed (Tillaux fracture) (2) or it ruptures.

33 Radiograph: Note in the lateral projection:
Note in the anteroposterior projection:
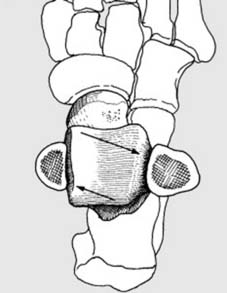
34 Supination/adduction injuries (adduction injuries) (a): The foot inverts, but the tendency to external rotation of the talus as a result of the torque convertor effect is countered by the direction of forces applied to the forefoot by the impact. The overall effect is adduction of the talus in the mortise. If the forces are slight, a partial tear of the lateral ligament results (sprain of ankle).



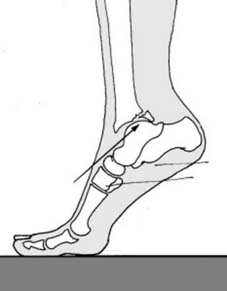
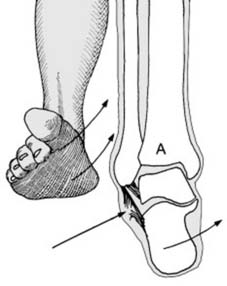
40 Pronation/dorsiflexion (compression injuries) (a): Commonly the foot is dorsiflexed at the ankle in association with an upward compression force – usually from a fall from a height or from a road traffic accident (A).



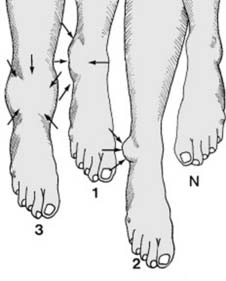
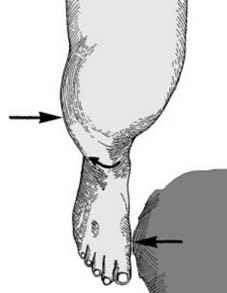
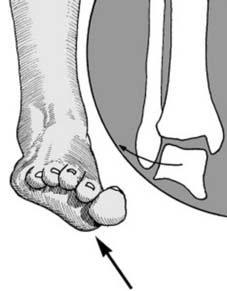
45 Diagnosis of ankle fractures: (a) Swelling: Note the site and distribution of swelling and bruising, e.g. (1) Diffuse swelling in front of the lateral malleolus in many ankle injuries. (2) Egg-shaped swelling over the lateral malleolus shortly after complete lateral ligament tears or lateral malleolar fractures (McKenzie’s sign). (3) Gross swelling and bruising in many trimalleolar and compression fractures. Swelling and bruising which involves both sides of the ankle is highly suggestive of an unstable injury.

Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


