CHAPTER 15 Individualized Unicompartmental Knee Arthroplasty
 Individualized UKA addresses anatomic differences between medial and lateral condyles regarding width, anterior length, and different anterior radiuses, as well as geometric differences between medial and lateral tibial plateaus.
Individualized UKA addresses anatomic differences between medial and lateral condyles regarding width, anterior length, and different anterior radiuses, as well as geometric differences between medial and lateral tibial plateaus.

Femoral Components
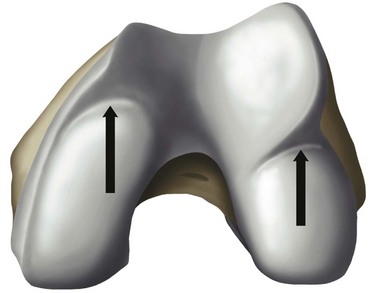
The overall goal of selecting a femoral component is optimal fit. The femoral component should not overhang, but it should be wide enough and match the geometry without impingement of the medial spine or the posterior cruciate ligament. The transition to the femoropatellar joint should be smooth, not prominent, and the femoral component should not be too long, specifically on the lateral side to avoid patellofemoral (PF) impingement. Hernigou and Deschamps1 reported on 99 unicompartmental arthroplasties (UKAs) with a mean follow-up of 14 years. Of these, 29% were symptomatic due to patellar impingement through the femoral component. In this group, lower Knee Society scores were related to problems climbing stairs. They proposed two failure mechanisms; one may be related to an over-resection off the posterior condyle, which consequently moves the femoral component more anteriorly. They also hypothesized that poor intraoperative judgment of the linea terminalis, which describes the trochleocondylar junction, could lead to oversizing the femoral component. Figure 15–1 shows the transition between the medial and lateral condyles to the trochlea. The linea terminalis is the result of the medial and lateral meniscal impression on the femur and can be seen on lateral radiographs. In Herningou and Deschamps’s series, the trochleocondylar junction was an average of 3 mm anterior on the medial and 4 mm posterior on the lateral side relative to a line representing the slope of the intercondylar roof.1 Berger et al.2 reported the results of 59 UKAs with a follow-up of 11–15 years. The main failure mode was symptomatic patellofemoral osteoarthritis in 10%; this was observed despite a pristine PF joint preoperatively. In a group of 48 living patients who had an average radiographic follow-up of 17 years, Squire et al. reported evidence of PF osteoarthritis in 35 patients (87%).3 A total of 14 knees were revised. Six patients were revised for disease progression, but it was not defined whether this was related to PF osteoarthritis.
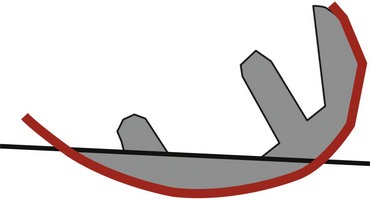
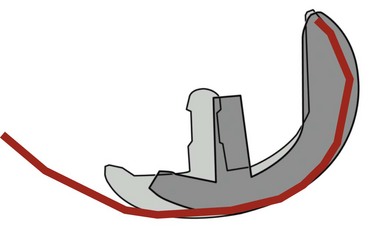
The linea terminalis has to be respected to avoid PF impingement. Both surgical technique and femoral implant design play a role. The distal femoral cut in most systems is not based on an intramedullary rod, but solely on the tibial cut. It is difficult for the surgeon to judge the correct amount of flexion of the distal femoral cut. This step determines the amount of flexion in which femoral component is implanted. If the knee is hyperextended, the distal femoral cutting block cuts in more extension. If the knee is held in more flexion, the component results in a more flexed position. However, the tibial cut can vary depending on whether there is more or less slope, which additionally contributes to more or less flexion or extension. Individualized femoral jigs may help to resolve this source of surgical error. Figure 15–2 shows a femoral component in too much flexion, resulting in PF impingement. All three studies cited above reported increasing PF osteoarthritis in the second decade. All studies used an only-femoral component (Fig. 15–3), which means that the anterior edge is not curved below the subchondral bone. This is in contrast to a recessed femoral component where the edge of the implant extends below the subchondral bone as shown in Figure 15–4. Using a recessed single-radius femoral component, progression of PF osteoarthritis was not seen in a series with a follow-up between 10 and 20 years.4 It remains unclear, since there is no reported 10- to 20-year follow-up series of a tapered J-curve design, whether this is related to the recesses design itself or to the single-radius design. The single-radius femoral implant restores the posterior condylar offset by balancing the flexion gap prior to the extension gap, so the surgical technique is very focused on restoring the posterior condyle. Additionally, its shorter design, replacing only the posterior condyle, may increase femoropatellar offset, which may result in decreasing PF stresses and thereby reducing the likelihood of PF osteoarthritis. However, since PF peak stresses are lowest in extension and increase during flexion,5,6 J-curve femoral components reconstructing the posterior condyle should achieve the same offset compared to a single-radius design (see Fig. 15–4). Restoring the cylindrical posterior condyle,7 therefore, should not result in significantly different PF stresses.

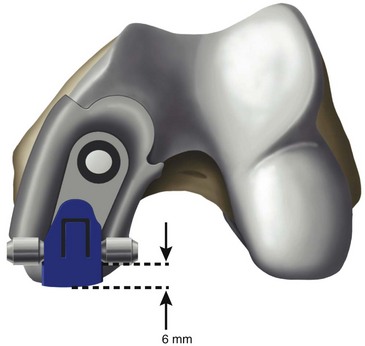
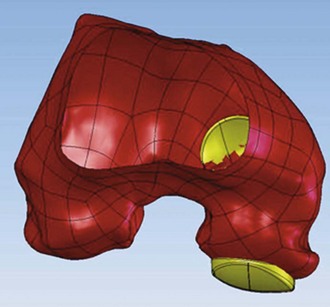
Only-femoral designs may be more susceptible to PF osteoarthritis as a failure mode in the second decade due to impingement between the patella and the edge of the femoral implant. This may be additionally enhanced with the decreasing of cartilage thicknesses as we get older. Individualized UKAs have several advantages compared to off-the-shelf implants: computed tomography (CT) data are utilized to identify the linea terminalis and the implant is designed with respect to the transition to the PF joint with short lateral and longer medial components. The length of the components is related to the restoration of the posterior condyle. A surgical plan provides detailed information on how much bone needs to be resected off the posterior condyle. An example of 6 mm of posterior condylar resection is shown in Figure 15–5. Therefore, an incidental too-anterior placement of the femoral component is addressed by preoperative planning, individualized femoral cutting blocks, and cross-checking through the correct amount of resected bone. In order to address the problem of PF impingement, the anterior edge is recessed below the subchondral bone. Figure 15–6 shows a three-dimensional model demonstrating this design feature.
Width
The medial condyle appears narrower and the lateral condyle wider. Some authors, such as Yoshioka et al.,8 could not find a difference. Others described a wider lateral condyle: Mensch and Amstutz9 described an average width of 26.6 mm for the medial condyle and 26.9 mm for the lateral condyle in 30 cadaver knees. Erkman and Walker10 studied 50 radiographed knees and found similar measurements, but values were 10% larger, suggesting magnification differences. We found an average medial condylar width of 26.1 mm (range, 21–32 mm) and an average lateral condylar width of 28.5 mm (range, 22–36 mm) on 48 CT scans.11 Our data are very similar to published data. Looking at off-the-shelf femoral components (Table 15–1), the width is narrower compared to the femoral condyles’ dimensions. This is necessary to allow the surgeon to find the best implant placement and fit, since the bone is cut to fit the implant. The advantage of individualized femoral components are wider femoral components. However, whether this will be an advantage resulting in better long-term results with less femoral loosening still has to be proven. There may, however, be an advantage in heavier patients in that a wider femoral component reduces the overall stresses on implant and fixation.
Table 15–1 Minimum and Maximum Widths of Currently Available U.S. Femoral Components
| Implant | Minimum Width (mm) | Maximum Width (mm) |
|---|---|---|
| Stryker Triathlon | 19.0 | 24.0 |
| DePuy HP | 18.0 | 25.0 |
| Zimmer HF | 21.0 | 26.0 |
| Smith and Nephew Journey | 18.0 | 25.0 |
| Biomet Oxford | 19.0 | 23.0 |
| Wright Advance | 19.0 | 22.0 |
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


