Individualized Anatomic Anterior Cruciate Ligament Reconstruction
Introduction
The anterior cruciate ligament (ACL) is a dynamic, neurovascularly rich structure
Distinct bundles function synergistically and in concert with other ligaments, meniscus, and capsular attachments to facilitate normal kinematics
Traditionally, only one of the two native ACL bundles has been reconstructed; this “single-bundle” reconstruction places the ACL in a nonanatomic position
Anatomic double-bundle reconstruction better re-creates the native knee kinematics and function
Patient Selection
ACL ruptures are secondary to noncontact trauma to the knee during cutting or pivoting sports
Audible pop, immediate effusion
Lachman and pivot-shift tests
Isolated ACL injuries typically involve both bundles, but in rare cases only one bundle may be torn
Isolated posterolateral (PL) bundle injury—Positive pivot shift test and negative Lachman test
Isolated anteromedial (AM) bundle injury—Positive Lachman test and negative pivot shift test
KT-1000 and KT-2000 arthrometer testing (MEDmetric) can assist with diagnosis.
Indications
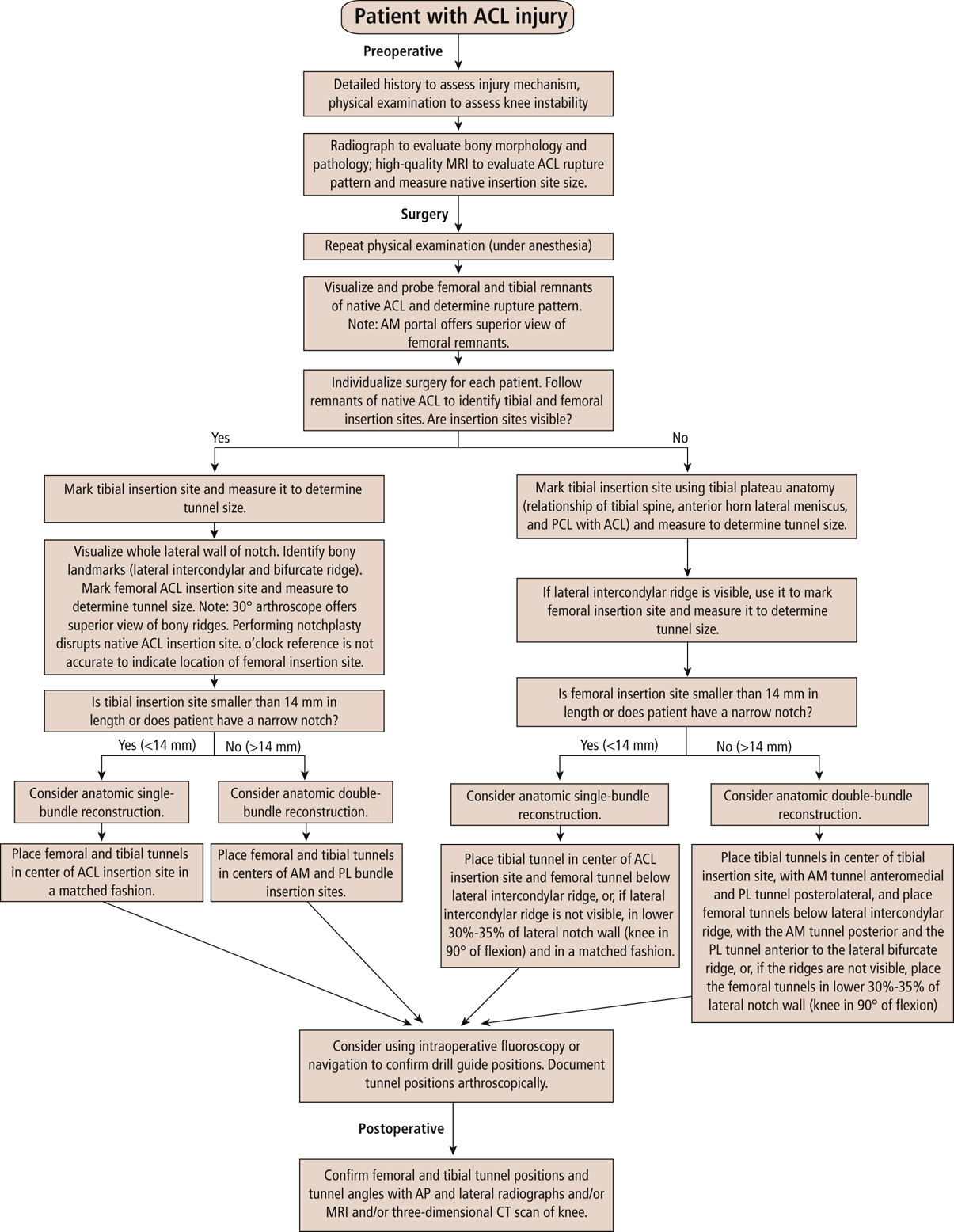
Figure 1Diagram depicts the algorithm used for anatomic single- and double-bundle ACL reconstruction. ACL = anterior cruciate ligament, AM = anteromedial, PCL = posterior cruciate ligament, PL = posterolateral.
(Adapted with permission from van Eck C, Lesniak B, Schreiber V, Fu F : Anatomic single- and double-bundle anterior cruciate ligament flowchart. Arthroscopy2010;26[2]:258-268.)
Indications for anatomic ACL reconstruction are well known and not discussed in this chapter
Use reconstruction algorithm for decision making on treatment (Figure 1)
Contraindications
Relative (as per senior author)
Small femoral or tibial insertion site; tibial site smaller than 14 mm will not support the necessary bone tunnels
Notch size less than 12 mm in medial-to-lateral dimension
Absolute
Active infection
Malalignment
If incompetent posterior cruciate ligament, posterior corner, or medial collateral ligament not addressed, the rate of failure of ACL reconstruction will increase
Preoperative Imaging
Radiography
Weight-bearing radiograph should be obtained
Evaluate for bony avulsions such as spine fractures or Segond fractures
Magnetic Resonance Imaging
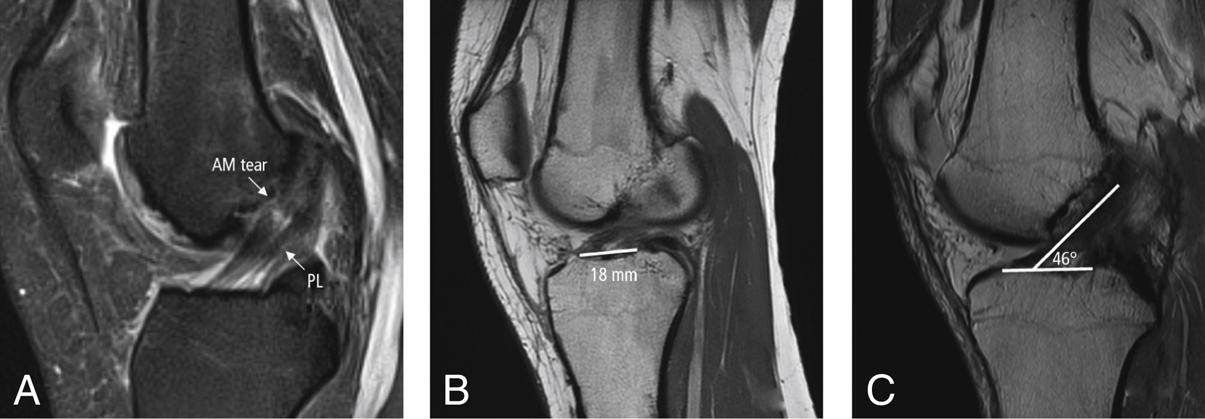
Figure 2Sagittal MRIs of the knee show a cut through the anterior cruciate ligament (ACL). A, The two-bundle anatomy of the ACL can be observed, as well as the presence of an isolated anteromedial (AM) bundle tear; the posterolateral (PL) bundle remains intact. B, The ACL insertion site is measured on MRI; it measures 18 mm in this patient. C, The inclination angle of the ACL is measured on MRI; it measures 46° in this patient.
Evaluate for concomitant ligament injury, meniscal pathology, or chondral injury
Preoperative planning of ACL bundles and insertion sites
Use oblique sagittal and oblique coronal planes to evaluate the AM and PL bundles
Can measure the ACL femoral and tibial insertion sites
Can determine autograft length and the diameter of the quadriceps and bone–patellar tendon–bone graft
Contralateral knee MRI can be used to measure native ACL inclination angle (Figure 2)
Procedure
Anesthesia
Regional used based on surgeon and anesthesia experience
Femoral and sciatic regional blocks frequently used, as well as spinal anesthesia
Examination Under Anesthesia
Passive range of motion (ROM) assessed; Lachman (translation and end point) and pivot-shift tests (compare with contralateral side)
Varus/valgus stability, dial test, posterior drawer test to evaluate other ligaments
Room Setup/Patient Positioning
Place tourniquet high on surgical extremity
Supine position with leg holder
Foot of operating table dropped to allow greater than 125° of knee flexion
Surgical Technique
Portals and Diagnostic Arthroscopy

Figure 3Photograph shows markings on the knee for the three-portal technique for anterior cruciate ligament reconstruction. The locations of the anterolateral portal (LP), the central portal (CP), and the accessory medial portal (AMP) are shown, as well as the location of the tibial incision for drilling the tibial tunnels and possible hamstring tendon harvest.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


