CHAPTER 22 Hybrid Arthroplasty
Two-Compartment Approach
 Hybrid arthroplasty allows surgeons to address medial and patellofemoral arthritis with a monolithic femoral component while maintaining both cruciate ligaments.
Hybrid arthroplasty allows surgeons to address medial and patellofemoral arthritis with a monolithic femoral component while maintaining both cruciate ligaments.

Setup and Equipment
Total knee arthroplasty (TKA) continues to be a safe and effective surgical procedure for arthritis of the knee, remaining the gold standard for treatment.1,2 However, from the author’s experience of performing TKAs for over 15 years, several observations are apparent. First, not all total knee replacement patients are happy with their postoperative function. The work of Phil Noble3 suggests that upward of 50% of TKA patients describe some form of functional deficit, particularly side-to-side movement. Such outcomes highlight the necessity of the anterior cruciate ligament (ACL) and how it may relate to functional satisfaction subsequent to knee arthroplasty. The second observation was that the ACL and the posterior cruciate ligament (PCL) were oftentimes healthy and undamaged at the time of the surgery. It was unsettling to realize that contemporary surgical techniques required the undue resection of these structures. The final observation was the documented combination of wear of the medial compartment and the patellofemoral joint (PFJ), coupled with a nonsymptomatic lateral compartment.4 Resection of the entire articular surface represented further unnecessary sacrifice of healthy tissue.
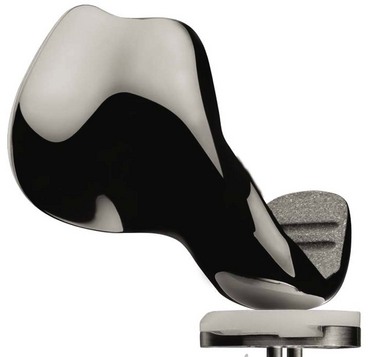
The idea of partial knee arthroplasty to allow retention of the lateral compartment and the cruciate ligaments is not new. Unicompartmental knee arthroplasty (UKA) and patellofemoral arthroplasty (PFA) have both been performed now for nearly 30 years.5,6 Replacing the medial compartment alone during UKA, while ignoring arthritic changes at the PFJ, has been recognized as a satisfactory surgical option.7 However, there is significant evidence that osteoarthritis (OA) may progress postoperatively, potentially compromising clinical outcome.8,9 One potential solution is the addition of a PFA to an existing UKA. However, mating these two implants can be technically challenging, via the introduction of three discontinuous zones between the articular cartilage and the implant. In addition to technical considerations, procedure cost must also be considered. The use of two procedures instead of one to address bicompartmental knee disease unnecessarily increases surgical cost. Seven years ago, a monolithic implant was designed to simultaneously replace the medial and the PFJ compartments of the knee (Journey Deuce Bi-Compartmental Knee System; Smith and Nephew, Inc., Memphis, TN) (Fig. 22–1). This device conserves both the ACL and PCL, in addition to sparing the nonsymptomatic lateral compartment. The all-polyethylene or metal-backed medial tibial baseplate is unicompartmental. Initial expectations included a smaller incision, potentially shorter recovery times postoperatively, less pain, reduced blood loss, and improved stability and function.
Approach
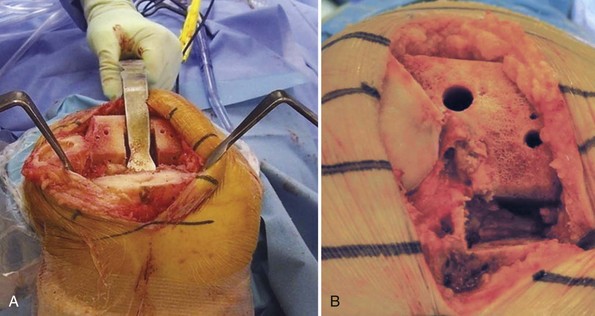
The development of less invasive arthroplasty techniques has been of interest for many years, despite concerns of reduced surgical visualization.10 Assuming relative ease of insertion and acceptable clinical outcomes, it is the author’s opinion that minimally invasive procedures are preferred. With the Deuce knee, the surgeon does not need to visualize the lateral compartment, other than momentarily to assess its integrity. The surgical technique allows for a relatively small incision and ease of insertion. Standard medial-parapatellar arthrotomy has been used for 80% of the author’s patients. Typically, this only involves a 1-inch split into the quadriceps. In 20% of patients, the author has used a midvastus approach without difficulty. This approach is typically reserved for those patients who have not undergone surgery previously, are less muscular, and are more flexible. When comparing the exposure of TKA to that of the Deuce knee, the potential benefits of this procedure are less dependent on incision length. Rather, the conservation of healthy tissue appears to be most important. Specifically, one is not exposing the lateral compartment or the lateral geniculate artery, which can increase pain and reduce postoperative function if not coagulated. Approximately 50% less bone is excised with the Deuce knee compared to traditional TKA. Moreover, the surgeon is able to avoid subluxing the tibia forward, placing a retractor in the lateral gutter, or everting the patella. The resulting reduction in blood loss and tissue tension may further improve postoperative surgical outcome. Surgeons are encouraged to make whatever exposure is necessary to perform the procedure without struggling, as incision length and violation of the quadriceps are not of primary concern with regard to recovery. Furthermore, liberal incision length may reduce risk of malalignment, skin slough, and retained cement.11,12 A comparison of TKA exposure versus that of the Deuce knee is provided in Figure 22–2.
 Technical Description (see Video 22-1)
Technical Description (see Video 22-1)
The technique for Deuce implantation begins with tibial preparation, which is similar to that of UKA. The Deuce tibial cutting block utilizes one pin to fixate the cutting block to the tibia, with a second pin utilized for fixation extending under the lateral tibial condyle. The initial pin is placed as a negative stop for the vertical and horizontal resection. This prevents stress risers under the tibial spine or in a vertical direction, helping prevent fracture. The two pins in these locations not only act to fixate the block but also avoid placement of pins in the subchondral bone, which could result in subchondral collapse of the tibial baseplate and subsequent failure of the procedure. A conservative tibial cut of 2–4 mm is made. In most instances, a resection of 2 mm off the lowest point of the tibial articular surface is ideal. If a neutrally aligned knee with medial and PFJ compartment wear exists, a 4-mm cut on the tibia is utilized to prevent overcorrection and overloading of the lateral compartment. A conservative tibial cut is recommended, allowing for neutral varus/valgus placement with a slope of 2–4°. Bicompartmental knee arthroplasty (BKA) with the Deuce knee has been shown to support knee alignment restoration.13 As with UKA, it is important to place the tibial base on the cortical rim without overhang, and to position the component as far laterally as possible without violating the ACL attachment on the tibia. This allows for maximal load to be distributed across the tibia. Spacer blocks allow for the determination of proper knee flexion and extension. Bone cuts similar to that for TKA are made, allowing for correction of extensive varus deformity. In contrast to UKA, balancing the knee in extension can be performed independent of flexion, supporting extensive deformity correction (Fig. 22–3).13,14 Mating the transition zone between the trochlea and lateral femoral condyle was the largest initial technical concern. With revised instrumentation, the author is able to make this process occur in a reproducible manner.
< div class='tao-gold-member'>

Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


