Fig. 3.1
An illustration adapted from Arthrotrain arthroscopic training module
3.2 Standardization of Training Centres
As the learning procedure is complicated and involves extensive equipment, expertise and provision of human tissues, it is recommended to observe the regulations accredited by the International Organisation for Standardisation (ISO). Reference can be made to the documents as enlisted in the appendant of the Orthopaedics Learning Centre, The Chinese University of Hong Kong (OLC). OLC has obtained the ISO9001 Certification, that the centre fulfils the requirements of a quality management system, which ensures that the centre can demonstrate the abilities to provide the products that meet the needs of customers consistently and to enhance customer satisfaction through an effective application of the system.
The ISO 9001 certification would ensure that the centre has done the right job, for the right person, in an effective manner.
Since human tissues are involved, it is important to pay attention to the procedures of procurement of the tissues, the regulations regarding handling of the tissues and the final dissemination of the remains to authorized centres. These are all outlined in the documents, Notes to participants: Precautions for Handling Workshop Cadavers (OLC) and Precautions for Handling and Disposal of Dead Bodies (Hospital Authority)
3.3 Design of a Training Programme
An arthroscopic training course should include five major sections:
- 1.
Basic didactic lectures of video to highlight specific clinical problems and arthroscopic anatomy setup of the operating theatre.
- 2.
Hands-on cadaveric demonstration and practice with preferably a 1:1 or 1:2 tutor–trainee ratio.
- 3.
Live surgery to illustrate key operating procedures to provide trainee surgeons real operating room experience.
- 4.
A full clinical round up with problem case discussion, round table quiz and a question and answer session. This will give a comprehensive approach to learning of skills, which is applicable to specific anatomical regions with clear illustration of major clinical problems.
- 5.
Feedback from trainees regarding the programme and tutors to improve the course.
Special anatomical regions may entail specific requirements pertaining to the unique clinical condition and skill training that matches the need to handle these conditions. Examples are illustrated as follows:
3.3.1 Knee
Knee arthroscopy technique has been widely applied in various areas including meniscal surgeries, ligament reconstructions, patellofemoral realignment surgeries, chondroplasty/microfracture surgeries and loose body removals.
A well-planned and thorough diagnostic arthroscopic examination should be conducted with visual feedback of the suprapatellar pouch, patellafemoral joint, medial and lateral gutters, medial and lateral compartments and the intercondylar notch region as well. Through workshop cadaveric training, participants would be allowed with the opportunities of mastering the three-dimensional fundamental technique of “triangulation” with one hand holding the arthroscope camera and other hand holding the instruments (Fig. 3.2).

Fig. 3.2
An illustration showing a knee cadaveric training station at work
The state of art of knee arthroscopy should focus on the establishment of portals and their trajectories to enhance subsequent instrumentations without causing hindrance. Needle technique gives surgeons and workshop participants a better sense of orientation prior portal establishment. The needle technique is even more crucial in establishment of posteromedial and posterolateral portals for difficult situations such as meniscal root tear surgeries and transtibial posterior cruciate ligament (PCL) reconstruction surgeries. Special precautions should be addressed on protection of vital structures particularly the popliteal neurovascular bundle.
The practice of knee arthroscopy should further include practice of meniscus procedures of various techniques in meniscal repair with regard to the meniscal tear configuration and the anatomical location. For ligament reconstructions, tunnel positioning and preparations with regard to the anatomical landmarks are to be demonstrated and practiced amongst surgeons.
3.3.2 Shoulder
The advancement of shoulder arthroscopic techniques enables surgeons to tackle simple procedures such as removal of loose bodies, bone spur removal, biceps tenotomy or tenodesis to more complex procedures such as rotator cuff repair, labral repair and acromio-clavicular joint excision or reconstruction.
The pros and cons of the beach-chair positioning versus lateral decubitus positioning and also the particulars with respect to traction should be reinforced. The orientation in each of the shoulder position should be clearly demonstrated with room allowed for practice. Skills in suture management, knot-typing and suture-passing techniques are essence of arthroscopic labral repair and rotator cuff repair (Fig. 3.3).
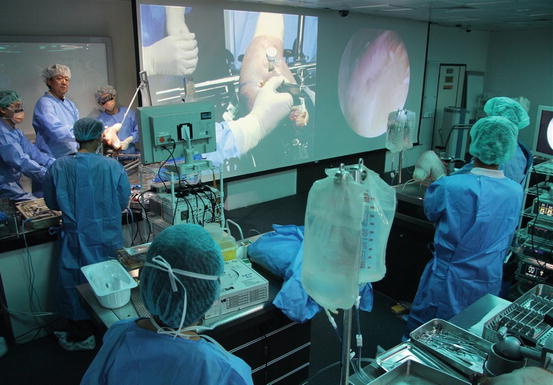
Fig. 3.3
An illustration showing how a teaching session on cadaveric model of the shoulder can be done in a lab setting with amplification to teach a bigger group of surgeons in training. This will give a “near-operating-room” experience followed by immediate practice on the cadaveric model with supervision of the mentor
3.3.3 Ankle
New techniques are emerging to deal with diverse ankle pathology. Those include deformity correction of hallux valgus, endoscopic superior peroneal retinaculum reconstruction, endoscopic calcaneofibular and anterior talofibular ligament reconstruction etc.
Related posts:
 Motor Learning Principles for Arthroscopic Motor Skill Teaching
Fundamentals of Being a Sport Surgeon
Setting Up a Curriculum
Motor Learning Principles for Arthroscopic Motor Skill Teaching
Fundamentals of Being a Sport Surgeon
Setting Up a Curriculum
 Simulators in Surgical Skills Training
Simulators in Surgical Skills Training
 Establishing Validation Methods: Measuring Progress (Measuring Teaching Effectiveness) – Global Rating Scales
Establishing Validation Methods: Measuring Progress (Measuring Teaching Effectiveness) – Global Rating Scales
 Arthroscopic Skills Training Modalities
Arthroscopic Skills Training Modalities
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


