How to Assess and Monitor Osteoporosis and Risk of Fracture
How to Assess and Monitor Osteoporosis and Risk of Fracture
Introduction
The aim in clinical practice is to identify those who are at high risk of fracture who will benefit from treatment. Is this high risk because of osteoporosis, high risk of falling, or a combination of both?
The ideal is to identify and treat before the first fracture, but for many the first suspicion of osteoporosis is raised by a long bone fracture following a fall or a spontaneous vertebral fracture. People sustaining a traumatic or low trauma fractures need to be assessed for the cause, in particular osteoporosis, to decide about the need for treatment to prevent another fracture. If osteoporosis is identified, then any underlying factors that may worsen the patient’s condition need to be recognized and managed. Finally, there is a need to monitor treatment to ensure the desired outcome is being achieved.
This chapter will attempt to answer these questions (Table 3.1) on a scientific basis, to give practical guidance for clinical management. Each medical unit will have to develop their own strategy from this for managing people with osteoporosis.
Assessing risk of osteoporosis and fracture
Fractures are increasingly common with ageing; one in three women and one in eight men over the age of 50 years will sustain a fracture. People who are osteoporotic are more at risk but not all those with osteoporosis will sustain a fracture during their lifetime and, conversely, not all those who fracture are osteoporotic. For a treatment that will prevent fracture, it must be targeted at those who are at greatest risk if it is to offer most benefit for that individual and to be cost-effective. The need is to identify those individuals who are at highest risk of fracture.
Table 3.1 Key clinical questions
Are they at high risk of future fracture?
Do they have osteoporosis?
If they have osteoporosis, is there a reason?
Was their fracture due to osteoporosis?
Was there any other reason why they sustained a fracture?
Do they need an intervention to reduce their risk of fracture?
What intervention is most appropriate?
Have they responded to treatment for osteoporosis?
Are they at less risk of fracture?
The risk of fracture can be expressed in terms of the probability of this happening in the following 10 years – the 10-year probability of fracture, given as a percentage or odds ratio. This timeframe is meaningful for the patient, and there is also evidence of the effectiveness of various treatments over this period of time.
The strongest risk factors for fracture are age and female sex. It is therefore appropriate to estimate the 10-year probability of fracture in those over 65 years, in particular in women. With an estimate of future fracture probability it will be possible to have an informed discussion about the potential benefits of any treatment. This is, however, only appropriate if the person is willing and capable to take a treatment long-term. Any decision by the person around this balance of risk and benefit will be influenced by other factors such as the individual’s personal experiences and subsequent anxieties about sustaining a fracture or suffering side-effects from treatment. It is not possible to predict for the individual whether they will sustain a fracture or benefit from a treatment, but we can estimate probabilities by the application of knowledge of the risk factors to the individual. Once the level of risk is estimated, it requires careful explanation to have any meaningful value for the patient.
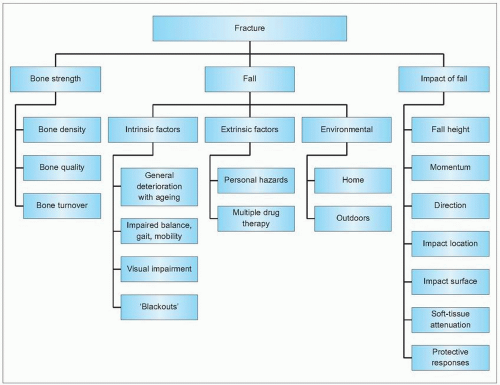
There are various factors that have been identified in epidemiological studies that are associated with an increased risk of fracture, in addition to age and sex (see Chapter 2), which can be used to aid this clinical decision-making process about whom to treat. These risk factors relate to bone strength, risk of falling, and the impact of any fall (3.1). Bone density has the strongest association with fracture risk, but no risk factor alone is of sufficient strength to identify those at highest risk in whom treatment to prevent fracture will be cost-effective.
3.1 Factors relating to risk of fracture.
Algorithms have, therefore, been developed to help identify those individuals most at risk (see Chapter 1 and vide infra). The algorithms rely on a combination of these clinical risk factors and assessing bone density when indicated. Such individuals will therefore gain most from any intervention, and interventions are also most cost-effective in this situation.
In practice when should risk of future fracture be assessed?
Those at highest risk are more likely to be identified if this is done later in life. The 10-year risk of fracture in a 50-year-old women is 9.8%, whereas it is 21.7% in an 80-year-old1. Fracture risk can be reduced within a year by various treatments in such older people. Such a ‘high risk’ strategy aimed at older people will prevent the greatest number of fractures and give the most personal and economic potential benefit.
Bone density measurement is not appropriate if a woman is premenopausal with no major risk factors as there is no proven specific intervention; general advice should suffice. However, it may be appropriate in a young woman with an eating disorder as this may influence her future behavior, or a person following transplantation or receiving high-dose corticosteroids as this may influence the use of a bisphosphonate. Compliance with treatment is generally increased following such informed decision-making. There is less of a reason to assess risk of fracture in perimenopausal women now that long-term hormone replacement therapy (HRT) is not considered appropriate as a routine way of reducing fracture risk.
Table 3.2 Clinical risk factors for osteoporosis and fracture
Clinical risk factors for osteoporosis and fracture
Age and female gender are the strongest risk factors for fracture. In addition, previous low energy fracture, glucocorticosteroid therapy, reduced lifetime oestrogen exposure, anorexia nervosa, low body mass index, maternal hip fracture, smoking, low levels of physical activity, and certain diseases such as rheumatoid arthritis and diabetes mellitus increase the risk of osteoporosis and fracture (Table 3.2). Although these factors are associated with increased personal risk, they cannot singly predict which individual will fracture, and are of limited value alone in deciding who will benefit most from an intervention. As risk of fracture is increased in those with clinical risk factors and low bone density, these clinical risk factors can be used to identify who should be assessed for their future risk of fracture by bone densitometry.
The absolute risk of fracture for any individual during the next 10 years will be a consequence of several of these factors, and the contribution to that absolute risk of each of these factors will vary. In an 80-year-old, age and risk of falling are most important, whereas in a 60-year-old, premature oestrogen deficiency and specific conditions such as steroid treated rheumatoid arthritis may be more relevant. The risk associated with some risk factors, such as smoking, is far less than the risk associated with others, such as associated with a previous low-energy trauma fracture. The goal is to develop algorithms that consider all the different risk factors and can enable a person to be given their 10-year probability of fracture. This work is ongoing.
In an individual over 75 years who has sustained a low-energy trauma fracture, the risk of future fracture is high enough that some guidelines, such as the NICE Guidelines in the UK, recommend treatment as it will be cost-effective to prevent further fracture. In younger people, other risk factors need to be present, including low bone mass, to identify those with a sufficiently high risk to justify treatment. (See also Table 2.13.)
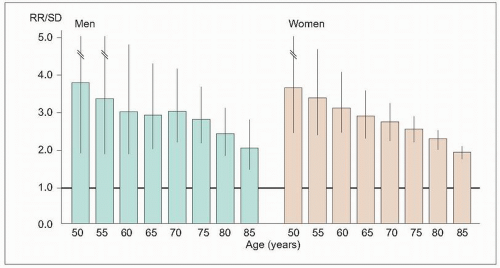
3.2 Bone mineral density at the hip is a strong predictor of hip fractures in both men and women. The risk is greater at 50 years than 80 years, as other factors become more important in the elderly. (Adapted from Johnell O, et al. (2005). Predictive value of BMD for hip and other fractures. J Bone Mineral Res20(7):1185-1194.)
Table 3.3 Bone density measurement: a comparison of methods (including qualitative parameters)
DXA of the hip is regarded as the golden standard and it is only DXA of the hip and spine that are thoroughly evaluated in relation to treatment, i.e. pharmacological trials with fracture as end-point
Bone mass measurements
The presence of osteoporosis can be determined by bone mineral density. The WHO definition of osteoporosis is based on measurement by dual energy X-ray absorptiometry (DXA) at the hip and lumbar spine. Bone mass accounts for 75-90% of the variance of bone strength, and for each decrease of 1 standard deviation in bone density at the proximal femur there is a 2-4-fold increase in fracture risk depending on age (3.2).
There are several methods of assessing bone mineral density (Table 3.3, 3.3–3.7). Measurement at any site is the best predictor of fracture at that site, the reason why DXA of the hip and lumbar spine are preferred. Measurement of the lumbar spine is best around 50-65 years, as vertebral factures are most common at an earlier age. The hip is more suitable in older people because the typical age of hip fracture is 80 years and because age-related degenerative changes of the lumbar spine result in overestimates in bone density. Measurement of the total hip by DXA is regarded as most reliable for monitoring bone mass, because of changes in disc spaces and joints of the lumbar spine with advancing age. The axial skeleton can also be assessed by quantitative computed tomography (QCT).
Only gold members can continue reading. Log In or Register to continue