Hip Arthroplasty via Small-Incision Enhanced Posterior Soft-Tissue Repair
Introduction
Small-incision enhanced posterior soft-tissue repair (SIEPSTR) is performed through a limited incision compared with the standard posterior approach
Involves meticulous reconstruction of posterior structures to reduce dislocation risk
No absolute contraindications; relative contraindications are the same as those for the posterior approach, including Parkinson disease, dementia, and inability to follow posterior hip precautions
Preoperative Imaging and Planning
AP pelvis
AP hip
Cross-table lateral hip
Preoperative templating and clinical examination determine the plan for leg length and offset
Procedure
Room Setup/Patient Positioning
Operating room table modified for posterior approach total hip arthroplasty (THA)
Lateral decubitus position using well-padded lateral hip positioner
Use an axillary roll
Pad all bony prominences
Test range of motion (ROM) to ensure that hip positioner does not interfere
Place bump under the knee
Palpate and mark greater trochanter
Surgical Technique: Total Hip Arthroplasty
 | Video 55.1 Noncemented Total Hip Arthroplasty via a Posterior Approach Using Enhanced Posterior Soft-Tissue Repair. William Macaulay, MD (16 min) |
Incision
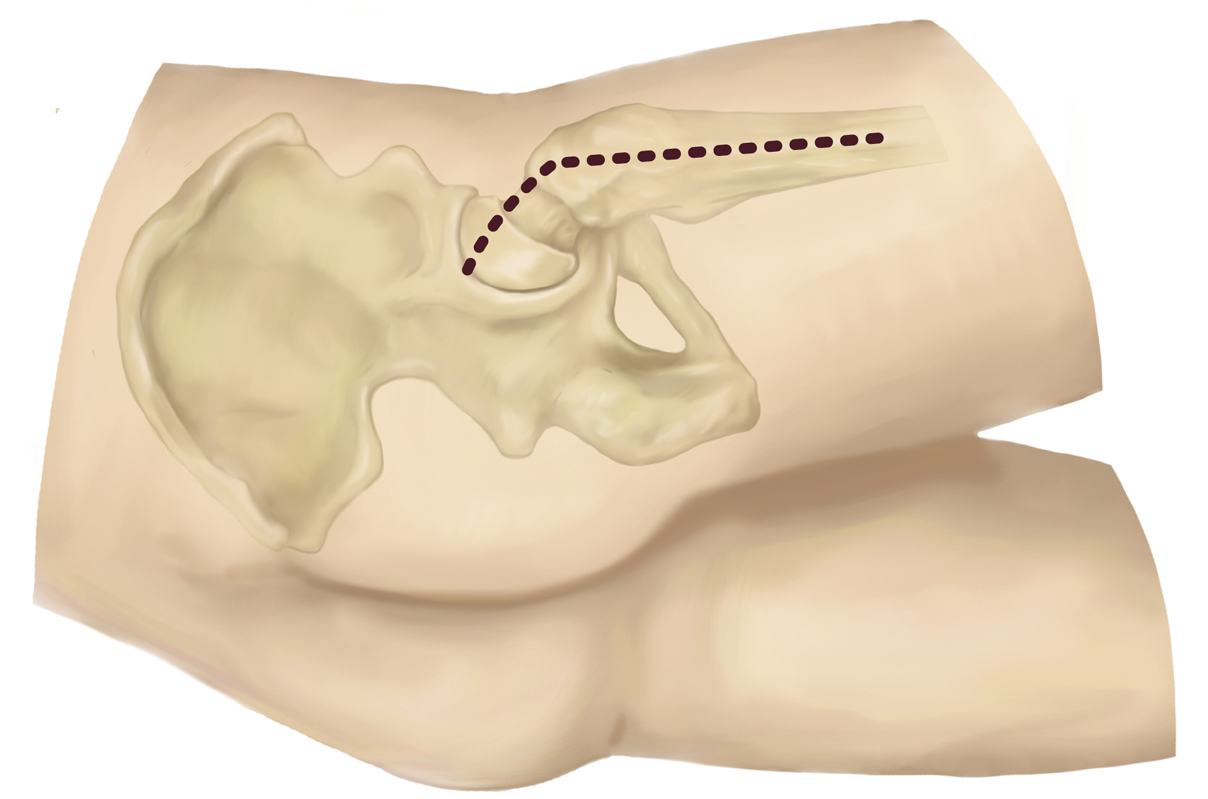
Figure 1Illustration shows the position of the planned incision for hip arthroplasty using the small-incision enhanced posterior soft-tissue repair (SIEPSTR) approach.
Draw a curvilinear incision with the distal portion centered over the lateral femur and curving posteriorly in line with the fibers of the gluteus medius once the incision reaches the tip of the greater trochanter. Approximately 2/3 of the incision should be distal to the tip of the greater trochanter, with 1/3 of the incision extending proximal (Figure 1)
Dissection
Sharply incise skin; coagulate bleeding vessels
Sharply dissect down to fascia lata
Incise tensor fascia over most prominent lateral aspect of greater trochanter
Use Mayo scissors to extend fascial incision distally and bluntly divide gluteus maximus muscle proximally using a finger
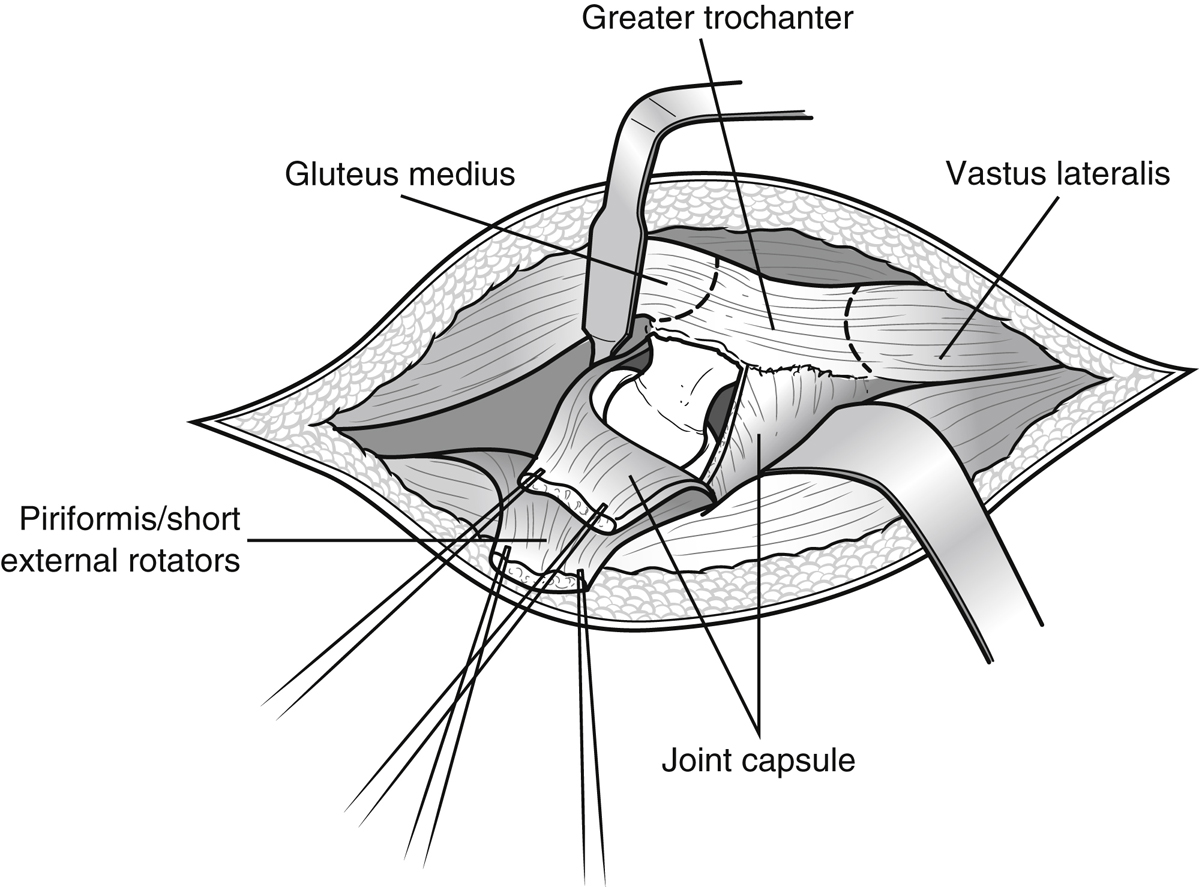
Identify short external rotators and place thin bent Hohmann “over the top” of piriformis to separate it from gluteus medius
Place Aufranc retractor on the capsule beneath the femoral neck
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


