Hip Arthroplasty via a Traditional and Minimally Invasive Direct Lateral Approach
Patient Selection
Indications
Primary and revision total hip arthroplasty
Hemiarthroplasty for displaced femoral neck fractures
Useful for patients with neuromuscular disorders, dementia, or alcoholism, because it reduces dislocation risk; also useful in those who cannot follow posterior hip precautions
Contraindications
High hip centers or hip dysplasia requiring access to superior acetabulum and ilium
Hardware removal or bone grafting requiring extensive dissection and exposure of the posterior wall or column
Preoperative Imaging
AP pelvis
AP and lateral hip
Cross-table lateral hip
Judet views or CT for abnormal anatomy (ie, dysplasia)
Procedure
Room Setup/Patient Positioning

Figure 1Illustration shows the use of a sterile drape bag to keep the ipsilateral leg sterile during hip arthroplasty via a direct lateral approach.
Lateral decubitus position with a lateral positioner
Use an axillary roll and pad all bony prominences well
Skin preparation and draping are done according to surgeon preference
Add a sterile leg bag to final drape anteriorly to patient to maintain sterility when dislocating surgical hip (Figure 1)
Surgical Technique: Total Hip Arthroplasty
 | Video 56.1 Total Hip Arthroplasty via a Direct Lateral Approach. Tahir Mahmud, BSc (Hons), MBBS, FRCS (Tr & Orth); Robert B. Bourne, MD, FRCSC (3 min) |
Surgical Approach
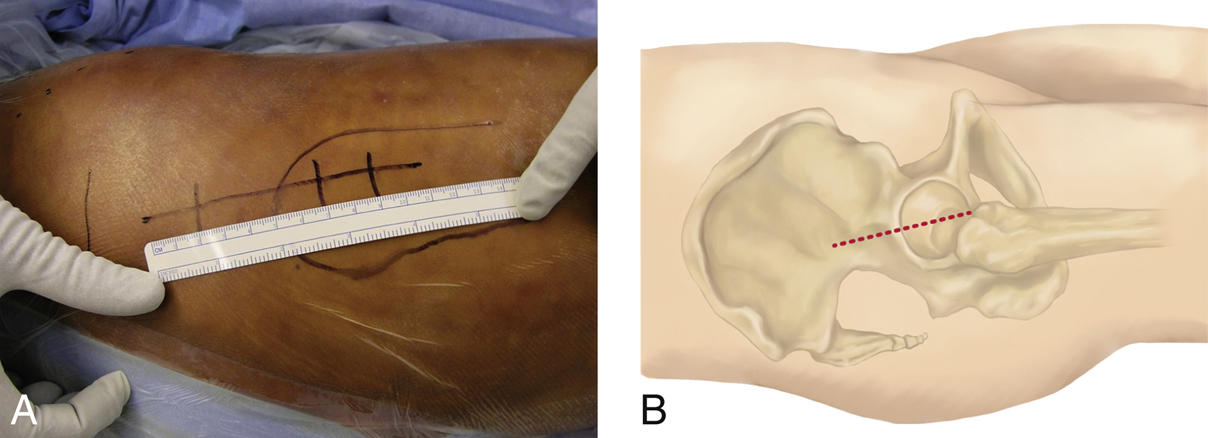
Figure 2Photograph (A) and illustration (B) show the skin incision for the direct lateral approach for hip arthroplasty. The incision is centered over the tip of the greater trochanter.
Mark greater trochanter on skin
Incision centered over the greater trochanter running obliquely from posterior proximally to anterior distally (Figure 2)
Dissection carried down to fascia lata using electrocautery
Identify and incise the fascia lata distally
A finger is inserted to develop the plane between the fascia and deeper musculature (vastus lateralis, gluteus medius) and the fascial incision is extended
Place Charnley retractor under anterior and posterior fascia lata to improve exposure
Exposing the Hip Joint
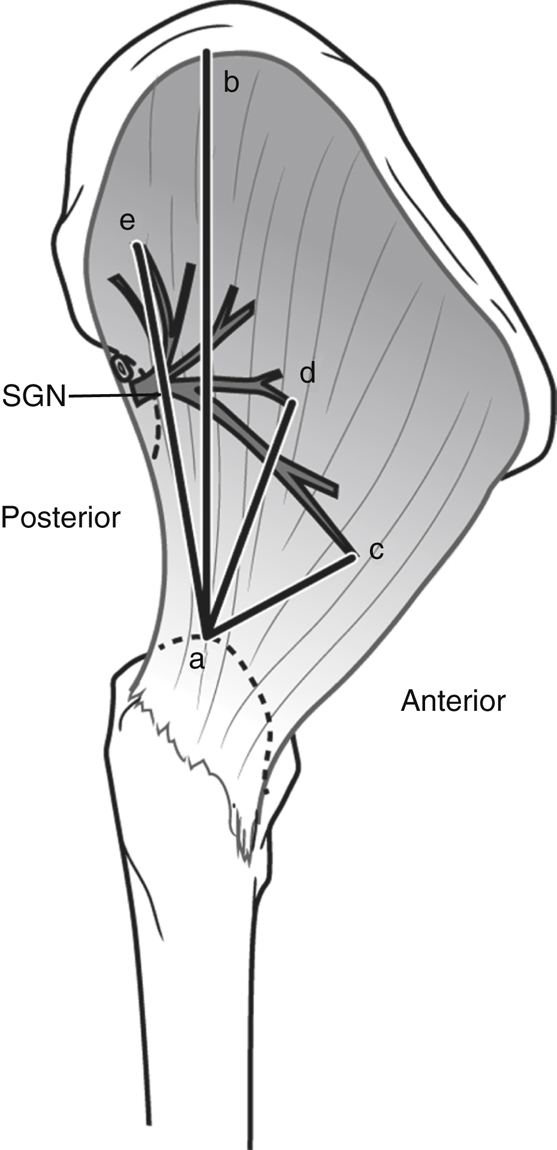
Figure 3Illustration depicts the relationship of the superior gluteal nerve (SGN) to the greater trochanter. a = tip of the greater trochanter; b = gluteal ridge; c = inferior branch of the SGN; d = middle branch of the SGN; e = superior branch of the SGN
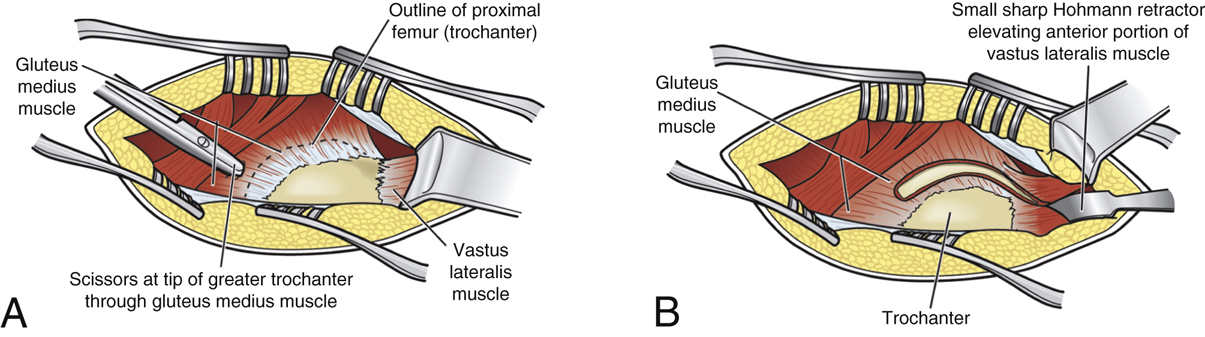
Figure 4Illustrations demonstrate exposure of the hip joint for total hip arthroplasty. A, The gluteus medius muscle is split carefully. B, An anterior sleeve consisting of the gluteus medius and minimus conjoined tendons is mobilized anteriorly.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


