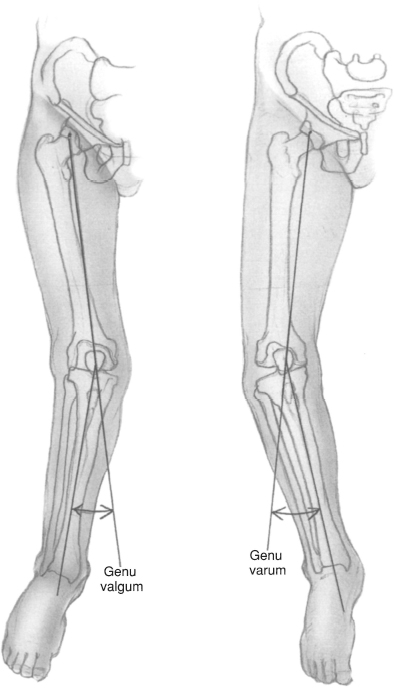
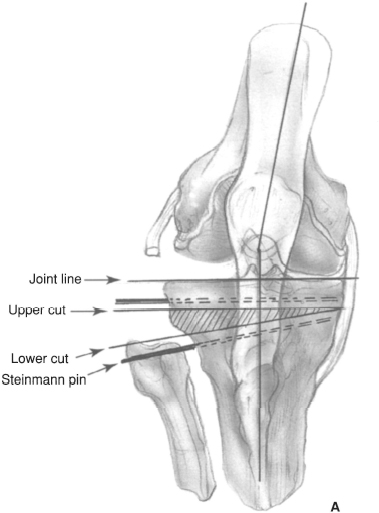
CHAPTER 28 Stephen G. Manifold and Giles R. Scuderi 1. Unicompartmental medial knee osteoarthritis 2. Age less than 50 years old 3. High activity level (e.g., heavy laborers) 4. Varus deformity 10 degrees or less 5. Flexion arc greater than 90 degrees 1. Rheumatoid arthritis or inflammatory arthritides 2. Flexion contracture greater than 10 degrees 3. Tibiofemoral subluxation (lateral) greater than 1 cm 4. Lateral thrust of knee during gait (high adductor moment) 1. Knee radiographs, including anteroposterior (AP), lateral, sunrise and standing three-joint films 2. Determine the femoral-tibial angle and the mechanical axis (Fig. 28–1). 3. Calculate the size of bone wedge to be removed from the proximal tibia. 4. Consider preoperative physical therapy to increase quadriceps strength and decrease flexion contracture. 5. Patient education to establish reasonable expectations 1. Supine position on a radiolucent operating table with a small padded bolster under the ipsilateral buttock. 2. The surgery can be performed with general, epidural, or long-acting spinal anesthesia. 3. Use basic orthopaedic instrumentation. 4. Use 1/8-in Steinmann pins, sharp straight osteotomes, and a sagittal saw. 5. Consider variable angle proximal tibia cutting guides to make accurate osteotomy cuts. 6. An L buttress plate should be available for fixation of the osteotomy site. 7. Use a fluoroscopic image intensifier for intraoperative imaging. 1. For patients without contraindications (i.e., significant peripheral vascular disease), a tourniquet should be placed as proximal as possible on the thigh to avoid minimizing the surgical exposure. 2. Intravenous antibiotics should be administered prior to inflation of the tourniquet. 3. A vertical skin incision is preferred in order to improve exposure for internal fixation and to facilitate possible total knee arthroplasty in the future. Figure 28–1 Genu valgum. The mechanical axis is defined as the intersection of a line drawn from the femoral head to the center of the knee and a second line drawn from the center of the knee to the center of the ankle. Genu valgum results in a “knock-knee” extremity alignment. Genu varum results in a “bow-legged” extremity alignment. Figure 28–2 (A) Osteotomy outline. Note the upper osteotomy cut is parallel to the joint line. The lower cut is just above the insertion of the pateltar tendon. Note the division of the tibiofibular syndesmosis. 4. The Steinmann pins should be positioned parallel in the lateral plane to avoid rotational problems after the osteotomy.
High Tibial Osteotomy
Indications
Contraindications
Preoperative Preparation
Special Instruments, Position, and Anesthesia
Tips and Pearls
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


