Hand Orthopaedic Tests
Hand Palpation
Anterior Aspect
Descriptive Anatomy
The thenar eminence lies at the lateral aspect of the hand with the palm facing out. It comprises three muscles that move the thumb: abductor pollicis brevis, opponens pollicis, and flexor pollicis brevis. These muscles are innervated by a branch of the recurrent median nerve (Fig. 8-1). Severe, prolonged compression of the median nerve in the carpal tunnel may cause the muscles of the thenar eminence to atrophy.
Procedure
Palpate the thenar eminence from the base of the thumb medial to the central aspect of the hand at the base of the carpal bones, then inferior and lateral to the base of the forefinger (Fig. 8-2). Look for hypertrophy or atrophy in comparison with the opposite hand. If atrophy or wasting is accompanied by pain and paresthesia along the medial nerve distribution, suspect compression of the medial nerve in the carpal tunnel.
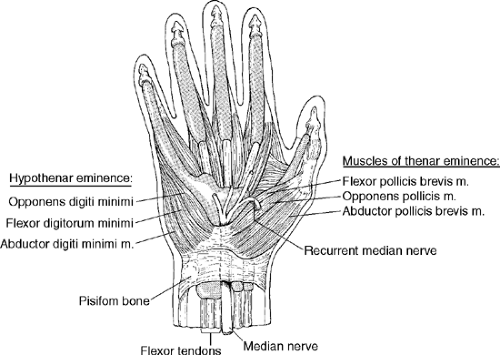 Figure 8-1 |
 Figure 8-2 |
Descriptive Anatomy
The hypothenar eminence lies at the anterior aspect of the hand from the base of the little finger to the medial aspect of the hand, ending at the pisiform (Fig. 8-1). This eminence contains the abductor digiti minimi, opponens digiti minimi, and flexor digiti minimi. These muscles are supplied by the deep branch of the ulnar nerve. Severe, prolonged compression of the nerve either in Guyon’s tunnel or more proximally in the extremity may cause wasting of the hypothenar eminence.
Procedure
Palpate the length of the thenar eminence from the base of the little finger to the base of the pisiform (Fig. 8-3). Look for hypertrophy or atrophy in comparison with the opposite hand. Wasting of the hypothenar eminence may indicate a compression of the ulnar nerve either in the tunnel of Guyon or more proximally in the extremity.
 Figure 8-3 |
Extensor Tendons
Descriptive Anatomy
The posterior aspect of the hand contains an intricate system of ligaments, fascial bands, and tendons—the extensor mechanism. This mechanism provides active extension to the fingers and contributes to the stabilization of the hand and digits. The extrinsic extensor tendons run along the entire length of the posterior aspect of the hand to each digit (Fig. 8-4). The tendons can be affected by trauma, which can strain or rupture them, and by rheumatoid arthritis, which can displace them.
Procedure
With the patient’s fingers and wrists extended, palpate the length of each tendon of the extensor digitorum communis from the base of the wrist to the proximal phalanx (Fig. 8-5). Note any tenderness, cysts, displacement, or loss of continuity of any of the individual tendons. Tenderness and displacement indicate rheumatoid arthritis. Loss of continuity secondary to trauma with loss of digit extension may indicate a ruptured extensor tendon. Small, easily palpable pealike cysts may develop between the second and third metacarpal bones.
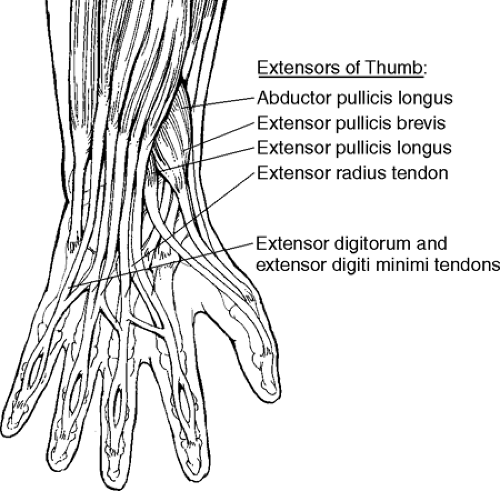 Figure 8-4 |
 Figure 8-5 |
Descriptive Anatomy
The metacarpal bones and phalanges are held together by a series of ligaments and joint capsules that supply stability to the joints (Fig. 8-6). The metacarpal and phalangeal bones are easily palpable from the posterior aspect of the hand. They are susceptible to traumatic fractures. The joints may become inflamed and are a common site for rheumatoid arthritis.
Procedure
Palpate each individual digit and metacarpal bone (Fig. 8-7). Look for tenderness, swelling, temperature differences, and bony nodules. Tenderness and swelling following trauma may indicate a fracture. Swelling around a joint capsule may indicate an inflammatory process, such as rheumatoid arthritis. Bony nodules (Heberden’s nodes) on the posterior and lateral surfaces of the distal interphalangeal joints may indicate osteoarthritis.
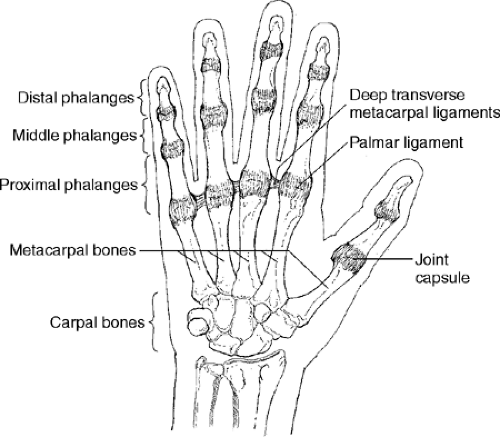 Figure 8-6 |
 Figure 8-7 |
Joint Instability
Description
The interphalangeal joints are the most common site of joint injuries to the hand. The injuries range from simple sprain to partial collateral ligament injury to dislocation to fracture–dislocation. Joint stability is maintained by the collateral ligaments in combination with the volar plate, which produces a three-sided box around the joints (Fig. 8-8). The most commonly affected joints are the index and little finger. Joint instability is usually due to dislocation.
Clinical Signs and Symptoms
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


