Introduction
Hamate fractures comprise two completely different fracture entities:
Type 1 Fractures of the hook of the hamate
Type 2 Fractures of the body of the hamate
All classifications divide hamate fractures into these two types.1,2 Some have subdivided type 1 fractures into tip of hook and base of hook fractures, which is of little clinical consequence. But dividing type 2 fractures (according to Hirano and Inoue2 ▶ Fig. 6.1) into 2a (coronal fractures) and 2b (transversal fractures) of the body of the hamate is of great clinical consequence. Type 2a (coronal) fractures of the body of the hamate are part of a fracture dislocation of the fifth carpometacarpal (CMC) joint (or the fourth and fifth CMC joints). The main consideration of treatment is the correct alignment of the fifth (and fourth) metacarpal. Type 2b (transverse) fractures of the body of the hamate are the “true” hamate fractures that will interfere with carpal biomechanics by breaking the carpal ring, and which need adequate stabilization. Isolated transverse fractures of the hamate are rare, but occasionally they occur as part of high-impact carpal injuries.
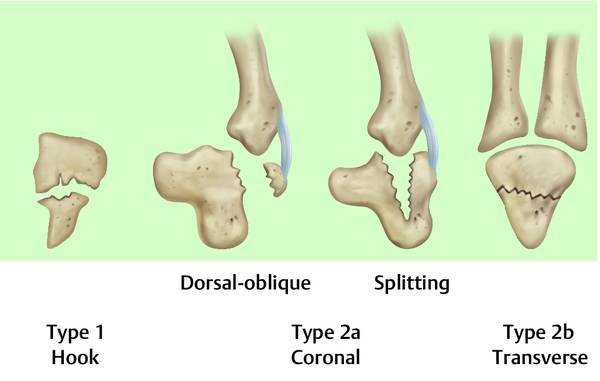
Fig. 6.1 Classification of hamate fractures according to Hirano and Inoue. (Reproduced from Hirano K, Inoue G. Classification and treatment of hamate fractures. Hand Surg 2005;10(2-3):151-157 with permission from World Scientific Publishing.)2
6.2 Hamate Hook (Hamulus) Fractures (Hirano Type 1 Fractures2)
Fractures of the hamate hook account for about 2% of all carpal fractures.3,4 The hamate hook (hamulus ossis hamati) marks the distal end of the ulnar border of the carpal tunnel. It acts as a pivot for the little finger and ring finger flexor tendons, which here are directed ulnarly toward their respective finger. The hamate hook is maximally loaded as a pivot in forceful grasping, with the wrist in ulnar deviation. Additionally, the pisohamate ligament transmits forces from the flexor carpi ulnaris tendon to the hamate hook. Thus, fracture of the hook of the hamate may be caused by a direct blow on the hypothenar, or by a sudden forceful pull of the flexor tendons, or by a combination of these. This may explain the high proportion of golfers and racket players among patients with hamate hook fractures.3,5
Clinical signs are tenderness and swelling at the ulnar base of the palm. The hook of the hamate pull test6 has proved valuable: With the hand in ulnar deviation, the patient pulls his or her flexed ring and little fingers against resistance, thus eliciting pain in the fractured hamate hook (▶ Fig. 6.2). Plain radiographs are taken to exclude adjacent injury, but they are not sufficient to diagnose or exclude hamate hook fractures, which are best diagnosed by CT (or newer MRT) scans (▶ Fig. 6.3).
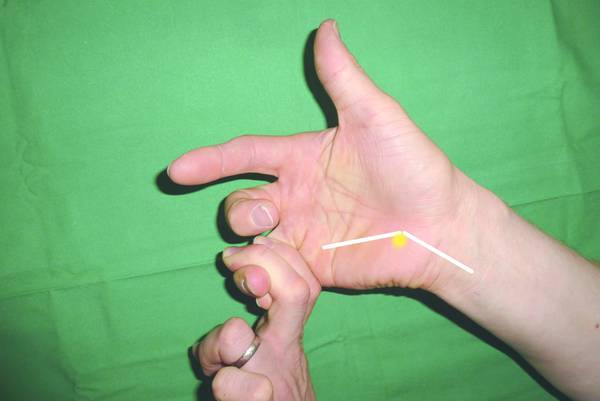

Fig. 6.3 CT scan of a fracture of the hamate hook.
Conservative therapy may be adequate in undisplaced acute fractures (less than 3 weeks after trauma), with application of a forearm cast for 6 weeks with the wrist in 15° flexion and 5° radial deviation (to reduce the pull of the flexor tendons from the hamulus).7 A high rate of pseudarthrosis has been reported after conservative therapy.5 So even if they are diagnosed early, surgery will be the preferred option for hamate hook fractures. Surgery is always indicated in late cases (>3 weeks after trauma) and in painful pseudarthroses.
Any surgery of the hamate hook puts the ulnar nerve at risk, in particular the deep (motor) branch of the ulnar nerve. From the view of a palmar approach, the main stem of the ulnar nerve passes over the tip of the hamate hook, whereas the motor branch spirals ulnarly around the hamate hook into the deep plane where it passes to the radial side of the hand over the metacarpal bases to the adductor pollicis and the thenar muscles (▶ Fig. 6.4).
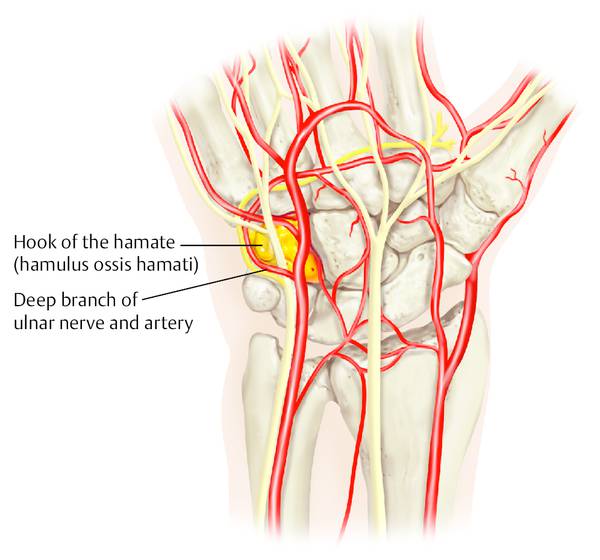
Fig. 6.4 The ulnar nerve passes over the tip of the hamate hook. The motor branch (deep branch) of the ulnar nerve spirals ulnarly around the hamate hook into the deep branch and is at risk in any hamate hook surgery.
Indirect surgery from the dorsum of the hand has been described using a leading K-wire and a cannulated screw,8 which may be safe in experienced hands. The author prefers the palmar approach. After opening the Guyon canal, the ulnar nerve and its motor branch are secured and the tip of the hook of the hamate is visualized. In acute fractures or delayed unions, the hamate hook is fixed with a 2-mm screw without opening the fracture site (▶ Fig. 6.5). As in every carpal fracture treatment, intraoperative X-ray fluoroscopy should be completed under forearm to-and-fro rotation, thus giving a good three-dimensional (3D) impression of the correct reduction and implant positioning.
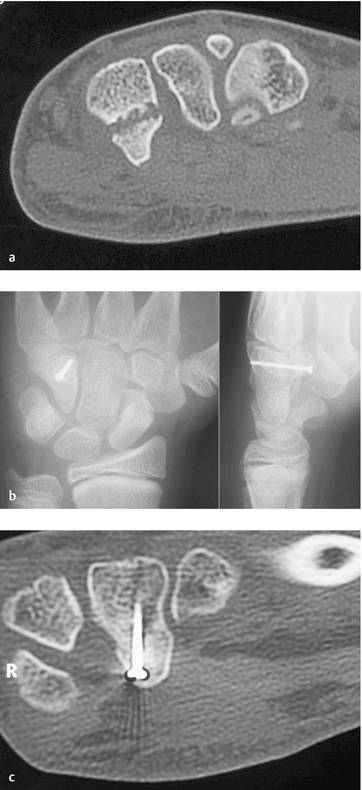
Fig. 6.5 Delayed union of a hamate hook fracture in a 12-year-old boy with persistent pain 8 weeks after a fall. (a) Only the CT scan visualized the diagnosis. (b) Radiography after open screw osteosynthesis from a palmar approach. (c
Related posts:
 Undisplaced Scaphoid Fractures
Undisplaced Scaphoid Fractures
 Proximal Row Fractures (Other Than Scaphoid and Pisiform Fractures): Triquetrum and Lunate Fractures
Proximal Row Fractures (Other Than Scaphoid and Pisiform Fractures): Triquetrum and Lunate Fractures
 Role of Hand Therapy in the Treatment of Distal Radius Fractures
Role of Hand Therapy in the Treatment of Distal Radius Fractures
 Intra-articular Fractures of the Distal Radius (AO type C3), (Dry) Arthroscopic Approach
Intra-articular Fractures of the Distal Radius (AO type C3), (Dry) Arthroscopic Approach
 Galeazzi Fracture-dislocation
Galeazzi Fracture-dislocation
 Unstable Ulnar Styloid Fracture
Unstable Ulnar Styloid Fracture
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


