In any practitioner’s repertoire of points GV-14 (da zhui) should come to the fore as a point of choice for strengthening the yang of the body if it is vacant or decreasing it if it is excessive. More times than not vacuity is our most common clinical scenario but both repletion and vacuity can manifest in patients so we should not forget this highly clinically effective point for those cases. This chapter addresses the treatment of GV-14 with the modalities of needling, moxibustion, bleeding, and cupping for the clinical manifestations of vacant or replete conditions. First, we will begin with a perusal of its clinical energetics in order to understand why it would be chosen as a point of treatment.
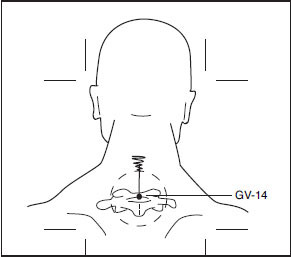
As a point on the Governing Vessel channel, the channel that governs the yang of the body, GV-14 has a role in regulating the yang. It is the meeting of all the yang channels. As such it strongly tonifies wei qi and stimulates the adrenal cortex. It opens to the exterior, opens the yang, clears the brain, and calms the spirit. It also can dramatically increase white blood cell production. It is viewed as an evil wind reflex, meaning this is a common area for entry of external wind. Governing Vessel 14 has been called the point of greatest yang in the body. Anatomically, it is located on the posterior aspect of the body, in the depression below the spinous process of the 7th cervical vertebrae, approximately at the level of the shoulder. If yang is vacant in a patient, this is an excellent point to needle or to apply moxibustion. If the yang is excessive, the point can likewise be needled, bled, and even cupped.
Such replete conditions include febrile disease, malaria, blood diseases, neck pain and rigidity, back stiffness, psychosis, epilepsy, seizures, pneumonia, schizophrenia, bronchitis, asthma, hepatitis, and eczema. In replete conditions the point must be needled obliquely upward to the standard depth of 0.5 to 1.0 cun with a dispersion technique such as a large amplitude and speed of rotation or with a vigorous lift/thrust needle technique with an emphasis on the withdrawal. Additionally, if there are heat manifestations such as fever, heat in the lungs, and labored breathing with yellow mucus as in the case of pneumonia, the point can be bled with a #28 g or #30 g filiform needle. Quickly insert the needle 0.01 cun into the point and obtain one to two drops of blood. This technique will reduce the heat/fire in the body. The application of a glass cup over the point after it has been bled will further expel blood to assist in a quicker resolution of the problem. Wear gloves when bleeding and/or cupping the point and sterilize all equipment properly after bleeding.
When the patient is vacuous, needling may also be employed using a tonification technique such as small amplitude of rotation and slow speed. Needle obliquely upward to the standard depth of 0.5–1.0 cun. Vacuity diseases include afternoon fever, pulmonary tuberculosis, cough, asthma, hemiplegia, pain in the back of the shoulder, tidal fever, hot sensation in the bones with recurrent fever, chills, and leucopenia (low white blood cell count).
Generous and frequent use of moxibustion may also be incorporated into the treatment to augment yang acuity. It is pleasant and soothing to the patient and has the known clinical efficacy of raising the white blood cell count. This is an excellent treatment for patients with weak immunity such as those with chronic fatigue, those undergoing chemotherapy, and patients with generalized kidney yang vacuity manifesting as low energy, desire to sleep a lot, cold hands and feet, and a tendency to catch colds easily. Moxa may be applied in any variety of forms that the practitioner prefers such as the moxa needle, indirect moxa pole, direct mini-thread moxa, tiger thermie warmer, or indirect moxa burner. Regardless of the form of delivery, administer the moxa for 3 to 5minutes per session. Treat subsequently according to signs and symptoms. Monitor for signs of heat aggravation and discontinue if they develop.
In cases of severe vacuity of kidney yang, abnormal neck pathology can develop—what can be called a fat pad at GV-14. As we have seen, da zhui is the point of greatest yang of the body. When the yang is severely vacuous, what might be called adrenal vacuity, this condition can present as a fatty pad at that point. The fat accumulation is evidence of the failure of the yang of the kidney to dominate water metabolism. The mound is water, tied up in the form of damp or fat. This condition should always be treated when you see the patient due to its clinical significance.
With the patient in a sitting position inspect the GV-14 area. The fat pad extends around this point in a round or oval-shape pattern. It is observed visually as a distinct mound. Further confirm this by grasping the area. Do not confuse this with a dowager’s hump. Patients who have the fat pad at GV-14 have other signs and symptoms of kidney yang vacuity such as excess weight, respiratory problems, loose stools with undigested food, lethargy, poor skin color, gas, abdominal distention, low blood pressure, cold feet, and more. Patients with hypothyroidism (kidney yang vacuity) present with this demarcation as well. Patients who have had a history of asthma or bronchitis, or those who have used steroids such as prednisone, may now suffer from adrenal insufficiency. Of all groups, the steroid users most frequently develop this distinctive feature.
Another disorder in which the fat pad develops is Cushing’s syndrome. Cushing’s syndrome is a disorder in which the face becomes fatter than usual, usually round and red. The body also becomes fatter, and often a pad of fat develops between the shoulder blades, making them look round-shouldered. At the same time muscle tone is lost from the arms and legs; they will feel weak, tired, their skin may become thinner and bruises sometimes appear spontaneously on the arms and legs. The bones become thin and fracture easily. Cushing’s syndrome is uncommon. It sometimes occurs in people on a long-term corticosteroid treatment.1
There is also what I call a preclinical fat pad that appears in the formative stages of kidney yang vacuity. The texture of the skin here is commonly thick or fatty. It is more characteristic of patients with a lesser degree of kidney yang vacuity than the more overt presentation that patients have with adrenal exhaustion. It should be treated in the same manner and its clinical significance is only one of degree.
Regardless of the diagnosis, to treat this problem grasp the area and insert a fine needle such as a #1 Seirin 40mm subcutaneously downward through the pad. Obviously, do not come out of the other side. Do not obtain qi but use a lift and thrust technique to stimulate the point. Retain the needle for 10 to 20 minutes. You may also use moxa around the borders of the area. Apply the moxa around the pad for about 3 minutes using a moving technique. The area should get mildly red. Figure 24.1 illustrates what the fat pad at GV-14 looks like and how the needle placement looks posteriorly, and Figure 24.2 shows a side view and how to needle it.
Related posts:
 Thoughts on Needling within the Clinical Encounter
The Role of the Heart in Needling within the Treatment Process
The Management of Multiple Sclerosis with the Extraordinary Vessels
Thoughts on Needling within the Clinical Encounter
The Role of the Heart in Needling within the Treatment Process
The Management of Multiple Sclerosis with the Extraordinary Vessels
 Prolapses: A Beneficial Treatment with Oriental Medicine
Prolapses: A Beneficial Treatment with Oriental Medicine
 The Ancient Use of ST-36 (Zu San Li) with Different Needle Techniques and Point Combinations
The Ancient Use of ST-36 (Zu San Li) with Different Needle Techniques and Point Combinations
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


