INTRODUCTION
Normal human locomotion has been the focus of intense clinical observational analysis for several decades. Through these efforts, the basic components of the gait cycle, its phases, and subphases have been identified, defined observationally, and linked to their kinematic, kinetic, and muscle behaviors. More in-depth analysis has revealed combinations of subphases that define the operational features of gait—organized components of the gait cycle reflecting functional features that achieve important operating objectives of the locomotion system. These objectives include advancement of the body’s center of mass by means of swing phase and stance phase propulsion mechanisms, foot–floor clearance mechanisms of the swinging limb, and antigravity stability mechanisms that operate during loading of body weight and the subsequent period of single limb support. Common gait deviations have also been analyzed in terms of how they relate to the larger context of the operational features of gait, providing insight into rehabilitative strategies that can best address operational features gone awry.
KEY CONTRIBUTORS TO HUMAN LOCOMOTION
This chapter describes human locomotion as a sequence of repetitive bodily motions organized functionally as a gait cycle. The chapter provides working descriptions of the gait cycle, its phases and sub phases, its kinematics, kinetics, and muscle kinesiology. Major objectives of the gait cycle are delineated including advancing the body’s center of mass, controlling upright stability against gravity and clearing the foot from the floor in order to avoid stumbling and falling. The chapter goes on to develop the concept of operational features of gait, namely, clinically observable components of the gait cycle that work together to achieve major gait objectives such as translation of the center of body mass and maintaining upright stability. Based on concepts developed in the paper, the chapter ends with case scenarios of patients with gait dysfunction that will hopefully alert the reader to useful ways of analyzing and treating problems of human locomotion. In analyzing human gait, the examiner must be knowledgeable about three contributors that have key roles in locomotion: ground reaction force, joint moments, and center of mass.
A force is a push or pull on an object that results from its interaction with another object. Forces result from interactions. Some forces result from contact interactions; normal, friction, and tension forces are examples of contact forces. Other forces are the result of interactions of the action-at-a-distance type (eg, gravitation and magnetic forces). According to Newton, whenever objects A and B interact with each other, they exert forces upon each other.
When a person stands on the floor, the body exerts a downward force on the floor (at minimum, the force of body weight). In a reciprocal manner, the floor exerts an upward force on the person’s body. Two forces result from this interaction: a force on the floor, and a force on the person’s body. These two forces are called action and reaction forces. Newton’s Third Law of Motion formally describes the relationship between these two forces: for every action, there is an equal and opposite reaction. To illustrate the concept of action–reaction forces, imagine preparing to get off a rowboat on a lake. What happens when we step off the rowboat onto the dock? As we move in the direction of the dock, the boat tends to move (accelerate) in the opposite direction. Acceleration is produced when a force acts on a mass.
What happens when we take a step on the ground? Does the ground move in the opposite direction (like the boat)? Physical analysis of this question involves Newton’s Second Law (F = ma), which describes the relationship between force, mass, and acceleration. The greater the mass of an object being accelerated, the greater the amount of force needed to accelerate that object. When we step off the rowboat onto the dock, the rowboat moves because its mass is relatively small. When we step on the ground, however, the mass of the earth is so large that the force exerted by the body against it can only minutely accelerate the earth. On the other hand, the body’s mass is small so that the reaction force of the earth, termed the ground reaction force, can easily accelerate the body. By Newton’s Third Law of Motion, the body’s pushing force on the earth is the same as the earth’s push back force on the body. Schematically, equation 1 below reflects the reaction force exerted by the earth on the person’s small body mass, resulting in a large acceleration. Equation 2 reflects the action force exerted by the person on the earth, resulting in a very small acceleration of the very large mass of the earth.
In summary, a person’s body has mass and, when the body stands on the ground, the body mass exerts a force on that ground. When the body exerts a pushing force on the ground, the ground exerts a push back force of equal magnitude on the body. This push back force is called the ground reaction force (GRF). When entities of different masses exert a force on each other, the entity with the smaller mass will have the larger acceleration. The ground reaction force is one of the keys to human locomotion because the smaller mass of the human body is easily accelerated by the ground reaction force during the gait cycle.
The fundamental objectives of human locomotion are to move the body’s mass from one place to another and provide antigravity stability so that a person doesn’t fall down. Locomotion mechanisms in the bipedal human are built around two facts: each lower limb is configured with many movable joints and, during walking, movements within and across each limb must be coordinated because both limbs are connected to the superincumbent mass by a pelvis. Translating body mass by means of bipedal locomotion depends on a repetitive sequence of joint motions that simultaneously move the body’s center of mass along an intended line of progression while counteracting the effects of gravity on upright posture and joint motion.
Movable joints in the walking human generate changing joint rotations that require control by muscular, soft tissue, and body weight forces. To understand how joint motion is controlled, we introduce the concept of joint moment, or force exerted by means of leverage. In general, a moment M is defined by a force exerted through a lever arm r, namely, M = rF (where force F is applied at a distance r from the axis of rotation). Figure 11–1 illustrates a person standing in equilibrium with a flexed knee. If unopposed by the quadriceps, body weight force (B) falling behind the knee would promote knee flexion collapse because of the rotary effect of joint moment Ba. The force generated by quadriceps contraction (Q) produces a counter joint moment, Qb. When Ba equals Qb, the system is in equilibrium and no motion occurs, all joint moments being perfectly counterbalanced. (Conversely, net unbalanced moments do result in joint motion, a finding characteristic of normal locomotion.)

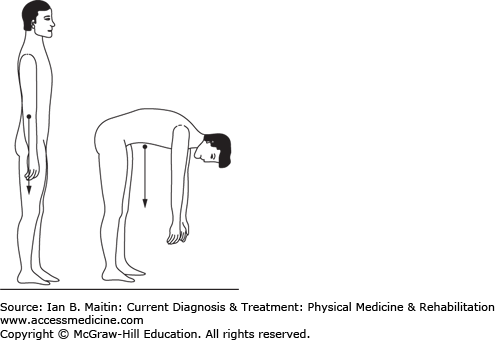
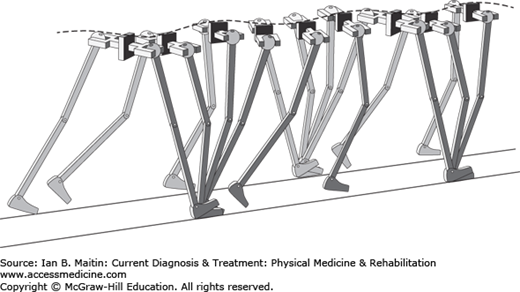
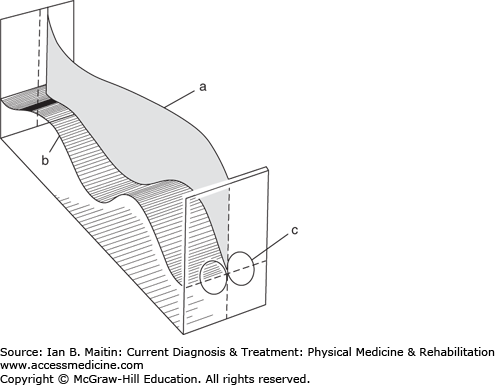
The center of mass (CoM) of any object is a point location where all of that object’s mass is imagined as concentrated. If we think of all bodily segments connected by joints as separate “objects” having their own CoM, we now assert that the CoM of the whole human body is that point in space where all joint moments created by the configuration of jointed body segments (ie, limb, trunk, and head postures) are in equilibrium. (Joint moments include all forces derived from muscle contraction, soft tissue resistance, and superincumbent body weight acting on the lever arms of their respective axes of rotation). As Figure 11–2 illustrates for a standing person, the location of the CoM is not a fixed point because it varies with body segment configuration. Similarly, as the body propels forward during ambulation, the CoM moves vertically and laterally; it does not behave as a fixed point. Viewed in the sagittal plane, the vertical displacement of the CoM moves as a smooth sinusoidal curve (Figure 11–3). This curve’s amplitude in a normal individual is approximately 5 cm (2 in.). The center of gravity also oscillates side to side during ambulation, generating another sinusoidal curve whose amplitude is approximately 6 cm (2.5 in.) (Figure 11–4). The significance of CoM motion for this discussion is that forces acting on the body during locomotion are conceptualized as acting through its CoM. In an upright standing human, the CoM is located just anterior to the S2 segment of the sacrum and, in general, during normal locomotion, it can be assumed to reside approximately there as well.
When a person stands, his or her body weight is applied as a force against the support surface of the ground and conceptualized as originating from the CoM. Newton’s Third Law states that when two bodies exert force on each other, these forces (termed action and reaction forces) are equal in magnitude, but opposite in direction. By this law, a reaction force is generated by the ground against the standing person’s body weight, the so-called ground reaction force (GRF). The GRF can be depicted as a vector having magnitude and direction. As a person walks and weight is shifted from one limb to the other, a series of GRFs are generated as weight is loaded onto, fully borne by, and then unloaded from each limb respectively and repetitively. GRFs can be measured in the laboratory using force plates situated in the lab’s flooring. Force plate output (normal and tangential shear forces) can then be processed electronically to generate a visible line superimposed over the video of a walking subject that represents the GRF vector in magnitude and direction. The GRF provides clinical information on magnitude and direction of joint moments for the weight-bearing limb as the vector passes anterior, posterior, lateral, or medial to the various joint centers of rotation. Many of the photographs and illustrations in this chapter depict the GRF generated by a subject walking in a gait laboratory.
PHASES & SUBPHASES OF GAIT
Human locomotion is characterized by a sequence of limb and trunk motions that have functional significance for advancing the body’s CoM and providing upright stability. The organized, complex sequence of joint motions inherent in walking has good repeatability and tight variability (ie, the standard deviation of gait parameters is small). Furthermore, bipedal human locomotion is a cyclical behavior, especially involving one or another lower limb maintaining contact with the ground at all times (Table 11–1).
| Term | Definition/Description | Example/Values |
|---|---|---|
| Gait cycle | Behavior that begins with an event involving one extremity and continues until the event is repeated once again with the same extremity. | |
| Stride length | One complete gait cycle. | The distance measured from a point on one foot to the same point on that same foot at the next stance. |
| Step | Activity that begins with an event involving one extremity and continues until the event is repeated with the contralateral extremity. | |
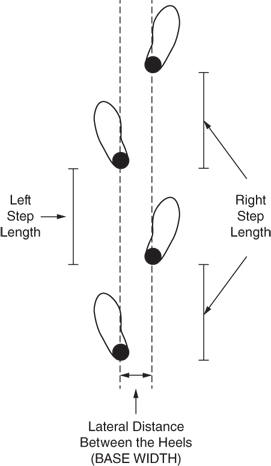
| Step length | Longitudinal distance between successive heel contacts of opposite feet; varies directly with height and inversely with age. | The distance measured during double support, from the foot that has just completed single support to the foot that has just completed swing. Left step length is measured when the left foot has just completed swing; likewise, right step length is measured when the right foot has just completed swing. |
 | ||
| Free velocity | Rate of ambulation chosen by a person when asked to walk comfortably; varies directly with height and inversely with age. | Normal adult = 80 m/min, 1.3 m/s, 4.3 ft/s, 3 mi/h; 90% of all individuals fall in the range 0.9–1.8 m/s (3.0–5.9 ft/s). |
| Cadence | The number of steps per unit time (1 min). | Normal adult = 90–120 steps/min. (See earlier figure.) |
| Base of support* | Mean lateral distance between the heels. | 90% of individuals fall in the range of 2.5–12.7 cm (1–5 in.). |
| Substitution mechanism | Motion used in an attempt to remedy the loss of one or another component of the normal gait pattern. | Circumduction is a mechanism used to achieve clearance when knee flexion or dorsiflexion is inadequate. |
| Open kinetic chain | Movement of a limb when the distal end is free to move in space. | The lower limb during the swing phase of gait. |
| Closed kinetic chain | Movement of a limb when the distal end is fixed. | The lower limb during the stance phase of gait. |
| Line of progression | Hypothetical line corresponding with the direction of walking. |  |
| Frontal view | As seen from the front or back. | |
| Sagittal view | As seen from the side. | |
The cyclical nature of gait, with its repetitive sequencing of joint motions, has led to eight descriptive functional units or subdivisions of the gait cycle, including two major phases, seven subphases, and one event. (Some authors do away with the term subphase entirely and refer to seven phases and one event). The two major phases, swing and stance, incorporate the seven subphases and one event, as discussed below.
Definition: The instant the foot contacts the ground (Figure 11–5).
Commentary: For normal locomotion with a continuum of gait velocities ranging between 0.9 and 1.8 meters per second (m/s), initial contact is characterized by a heel strike. At initial contact, the GRF generates three joint moments: ankle plantar flexion, knee extension, and hip flexion.
Ankle: At initial contact, the ankle joint is about neutral, held there by contraction of dorsiflexor muscles of the foot. The GRF falls posterior to the ankle joint axis, resulting in a plantar-flexion moment that leads to subsequent plantar flexion of the ankle.
Knee: At initial contact, the knee is fully or almost fully extended, the quadriceps muscle is active and acts to absorb the shock of heel strike, and the GRF falling anterior to the knee also contributes to preventing sudden knee flexion collapse resulting from the abrupt impact of heel contact with the floor, especially at higher gait velocities.
Hip: The hip at initial contact is flexed 30 degrees. With the GRF falling anterior to the hip and creating a flexion moment, previous muscle activity of the hamstrings that has helped to decelerate the swinging limb now helps to control the hip’s flexion moment at initial contact, taking note that gluteus maximus and adductor magnus contraction are only just beginning to activate.
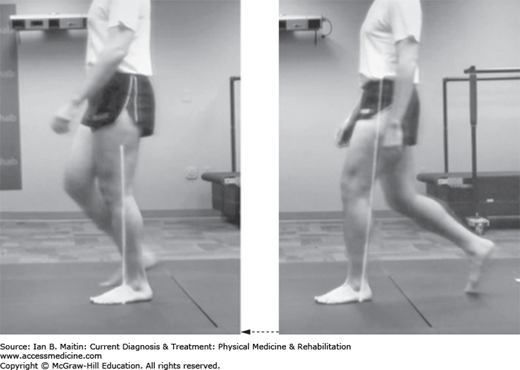
Definition: Shifting body weight onto the stance limb immediately following initial contact (Figure 11–6, right) to lift of the opposite extremity (Figure 11–6, left).
Commentary: Loading response reflects the shift of body weight from the contralateral support limb to the new support limb. During the loading response subphase, a period of double support exists because both limbs are actually in contact with the ground until the contralateral limb is lifted off.
Ankle: The loading response subphase begins immediately after initial contact and, at the ankle, is marked by gradual plantar flexion of 15 degrees, controlled by activity of the pretibial muscles (tibialis anterior, great and long toe extensors, and peroneus tertius). Heel strike may be heard but, normally, controlled plantar flexion prevents foot slap. The GRF falls posterior to the ankle joint (see Figure 11–6).
Knee: During the loading response, a flexion joint moment occurs at the knee, the GRF falling posterior to the knee joint. Eccentric contraction of the quadriceps group controls the rate at which the knee flexes. Contraction of the hamstrings quiets down as their role in decelerating the swinging limb comes to an end. At end of the loading response, the knee is flexed approximately 15 degrees.
Hip: Hip flexion of 30 degrees remains fairly constant throughout loading response. The GRF, initially anterior to the hip at initial contact, moves closer to the hip’s axis of rotation during the loading response. This reduces the effect of the hip flexion moment that is present at the instant of initial contact. Restraint of the hip flexion moment is provided by the gluteus maximus and adductor magnus. The activity of both of these muscles increases after initial contact while activity of the hamstrings deactivates.
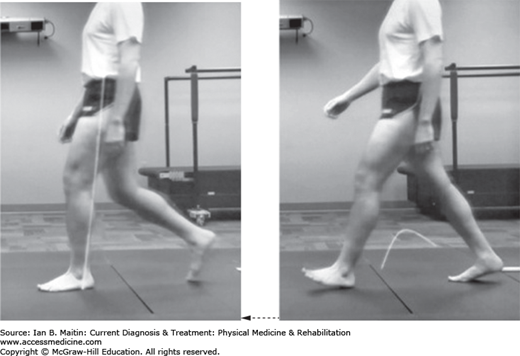
Definition: Lift of the contralateral extremity (Figure 11–7, right) to a position in which the body is directly over the stationary foot (Figure 11–7, left).
Commentary: In normal locomotion, lift of the contralateral extremity occurs concurrently with toe-off, especially the great toe. When the contralateral toes come off the ground, the period of ipsilateral single limb support of body mass begins. During midstance, the foot maintains contact with the ground throughout the entire subphase.
Ankle: At the onset of midstance, the ankle remains slightly plantar flexed (about 5 degrees). As the period of midstance develops, ankle movement to about 5 degrees of dorsiflexion materializes. The GRF moves over the forefoot as the tibia progresses forward (see Figure 11–7). With the GRF now anterior to the ankle, a dorsiflexion moment takes effect, reflecting forward acceleration of the tibia. This moment is controlled by activity of the soleus. However, gastrocnemius activity also contributes to attenuating the dorsiflexion moment that controls the rate of advancement of the tibia.
Knee: Maximum stance phase knee flexion is present at the beginning of midstance. During this subphase the knee undergoes extension by virtue of active quadriceps contraction. By the middle of midstance, the GRF moves just anterior to the knee joint’s axis of rotation, resulting in an extensor joint moment. Therefore, at the end of midstance, there is no longer any need for quadriceps activity as extension stability is provided passively by bony segment alignment and posterior soft tissue structures.
Hip: During midstance, the hip progressively extends as the tibia and femur advance forward. In the early part of the subphase, the hamstrings (semitendinosus and semimembranosus) contribute to extension, but, by late midstance, no further muscular effort is required. During the single support of midstance, the weight of the contralateral swing limb causes the pelvis on that side to drop about 4 degrees. The hip abductors, chiefly gluteus medius, are responsible for preventing excessive pelvic tilt.
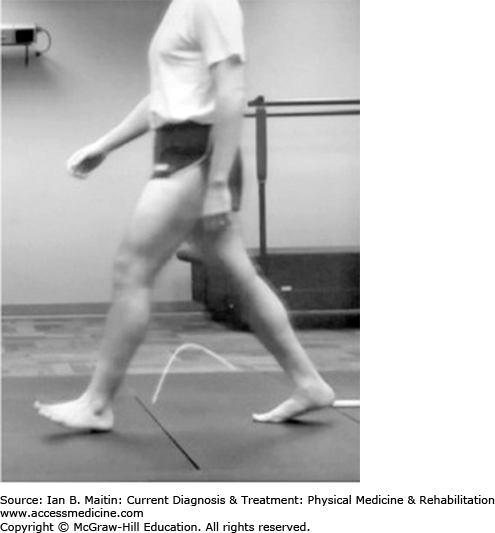
Definition: Subphase immediately following the position in which the body is directly over the stationary foot (Figure 11–8, right) to a point just prior to initial contact of the contralateral limb (Figure 11–8, left).
Commentary: The main force of propulsion advancing the body forward occurs during terminal stance. As the tibia continues to rotate forward in early terminal stance, buildup of calf muscle tension soon raises the heel off the ground. The GRF moves well into the forefoot and the CoM follows its sinusoidal path, descending from its high point at the end of midstance.
Ankle: In early terminal stance, the ankle continues to dorsiflex approximately 10 degrees, allowing the tibia to rotate forward. Calf muscle contraction subsequently intensifies and the heel rises. Dorsiflexion motion gives way to plantar flexion such that by the end of terminal stance (ie, the end of single support), the ankle reaches about 5 degrees of plantar flexion. The GRF has moved well anterior to the ankle joint along the forefoot (resulting in a long lever arm) so that strong contraction of both the soleus and gastrocnemius muscles is able to accomplish heel rise and control the dorsiflexion moment generated by the GRF. Heel rise also initiates dorsiflexion at the metatarsophalangeal joints. When body weight is transferred to the contralateral limb, calf muscle contraction deactivates quickly.
Knee
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree






